Department of Dermatology, Xiangya Hospital, Central South University, Changsha, China.
National Engineering Research Centre of Personalized Diagnostic and Therapeutic Technology, Changsha, China.
Front Immunol. 2023 Sep 20;14:1227905. doi: 10.3389/fimmu.2023.1227905. eCollection 2023.
Nirmatrelvir has been authorized for the treatment of both hospitalized and non-hospitalized COVID-19 patients. However, the association between T lymphocyte subsets and the outcome of hospitalized COVID-19 patients treated with oral Nirmatrelvir has not been investigated. The objective of this study was to examine whether lymphocyte subsets could serve as biomarkers to assess the risk of mortality in COVID-19 patients undergoing Nirmatrelvir treatment, with the aim of enhancing medication management for COVID-19 patients.
We conducted a retrospective cohort study at the Xiangya Hospital of Central South University in China between December 5, 2022 and January 31, 2023. The study reported demographic, clinical, T lymphocyte subsets, and inflammatory cytokine data of COVID-19 patients. We evaluated the associations of T lymphocyte subsets on admission with the composite outcome or death of patients using univariate and multivariable Cox regression analyses with hazards ratios (HRs) and 95% confidence intervals (CIs).
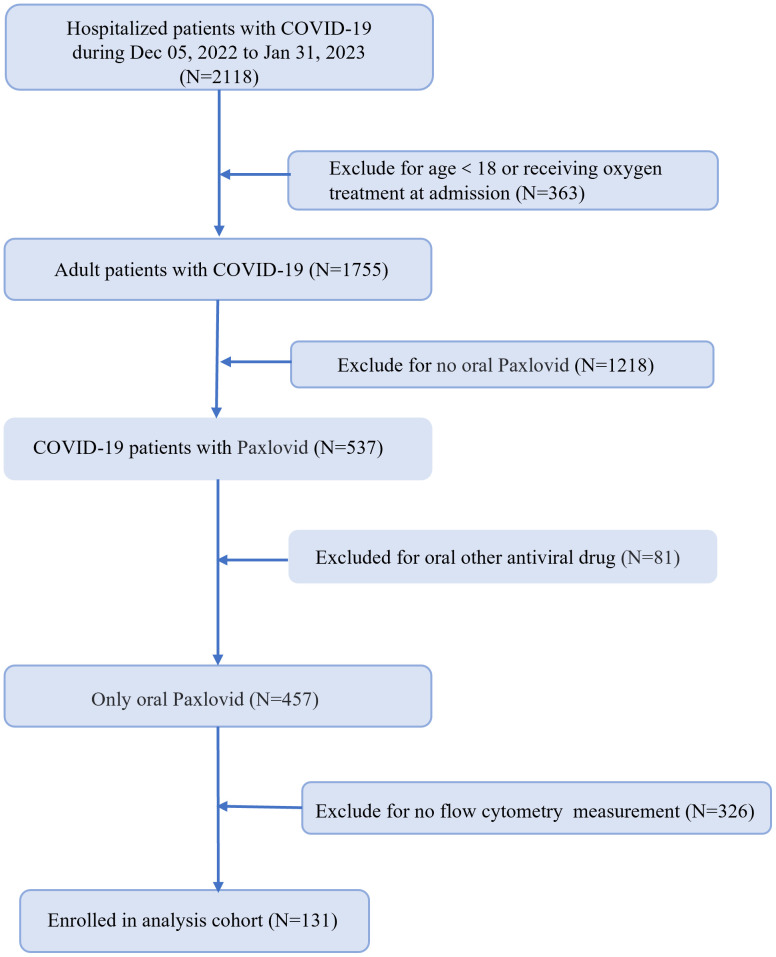
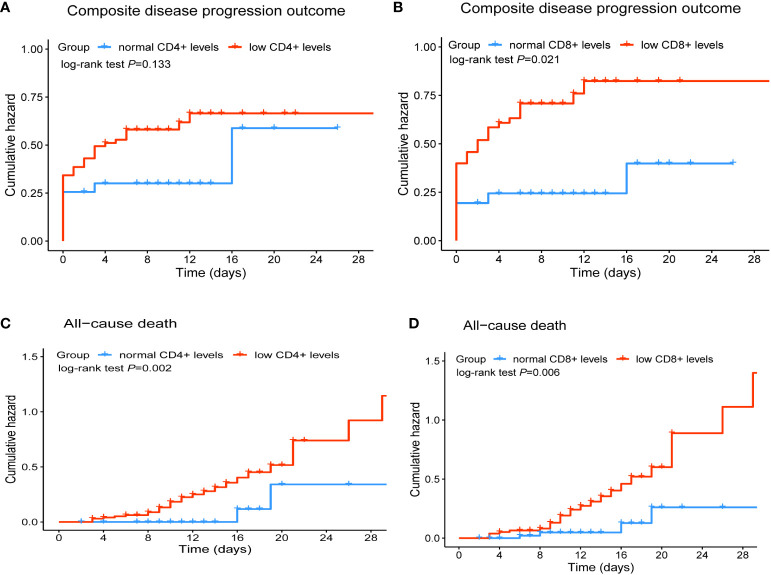
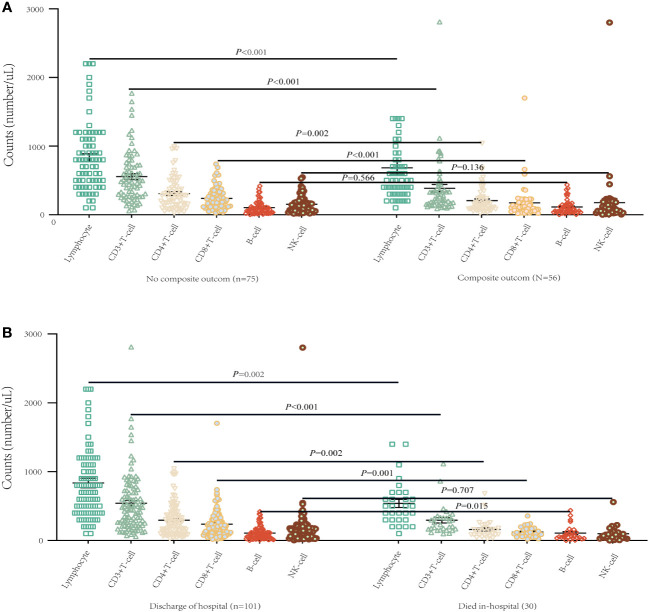
We identified 2118 hospitalized COVID-19 patients during the study period, and conducted a follow-up of up to 38 days. Of these, 131 patients received Nirmatrelvir, with 56 (42.7%) in the composite outcome group, and 75 (57.3%) in the non-composite outcome group. Additionally, 101 (77.1%) patients were discharged, while 30 (22.9%) died. Our results showed a significant decrease in the CD3+, CD4+, and CD8+ T cell counts of patients in the composite outcome group and mortality group compared to the non-composite outcome group and discharged group, respectively. Multivariate Cox regression analysis showed that the significant decrease in CD8+ T cell count in peripheral blood was independently associated with the composite outcome in COVID-19 patients treated with Nirmatrelvir, with an HR of 1.96 (95%CI: 1.01-3.80). The significant decrease in CD4+ and CD8+ T cell counts in peripheral blood increased the hazard of developing mortality, with HRs of 6.48 (95%CI: 1.47-28.63) and 3.75 (95%CI: 1.27-11.11), respectively.
Our study revealed a significant positive correlation between a decrease in CD8+ T cell counts and progression and mortality of hospitalized COVID-19 patients treated with Nirmatrelvir. Lower counts (/μL) of CD8+ T cell (<201) were associated with a higher risk of in-hospital severity and death. Our findings may provide valuable references for physicians in optimizing the use of Nirmatrelvir.
尼马曲韦已被授权用于治疗住院和非住院的 COVID-19 患者。然而,口服尼马曲韦治疗的住院 COVID-19 患者的 T 淋巴细胞亚群与结局之间的关系尚未得到研究。本研究的目的是探讨 T 淋巴细胞亚群是否可以作为生物标志物,用于评估接受尼马曲韦治疗的 COVID-19 患者的死亡风险,从而加强 COVID-19 患者的药物管理。
我们在中国中南大学湘雅医院进行了一项回顾性队列研究,时间为 2022 年 12 月 5 日至 2023 年 1 月 31 日。该研究报告了 COVID-19 患者的人口统计学、临床、T 淋巴细胞亚群和炎症细胞因子数据。我们使用单变量和多变量 Cox 回归分析,评估入院时 T 淋巴细胞亚群与患者复合结局或死亡的相关性,使用风险比(HR)和 95%置信区间(CI)。
我们在研究期间确定了 2118 例住院 COVID-19 患者,并进行了长达 38 天的随访。其中,131 例患者接受了尼马曲韦治疗,56 例(42.7%)患者出现复合结局,75 例(57.3%)患者未出现复合结局。此外,101 例(77.1%)患者出院,30 例(22.9%)患者死亡。我们的结果显示,与非复合结局组和出院组相比,复合结局组和死亡组患者的 CD3+、CD4+和 CD8+T 细胞计数显著下降。多变量 Cox 回归分析显示,外周血中 CD8+T 细胞计数的显著下降与接受尼马曲韦治疗的 COVID-19 患者的复合结局独立相关,HR 为 1.96(95%CI:1.01-3.80)。外周血中 CD4+和 CD8+T 细胞计数的显著下降增加了发生死亡的危险,HR 分别为 6.48(95%CI:1.47-28.63)和 3.75(95%CI:1.27-11.11)。
我们的研究表明,CD8+T 细胞计数的下降与接受尼马曲韦治疗的住院 COVID-19 患者的病情进展和死亡率呈显著正相关。CD8+T 细胞计数较低(/μL)(<201)与住院严重程度和死亡风险增加相关。我们的研究结果可能为医生优化尼马曲韦的使用提供有价值的参考。