Armstrong April W, Warren Richard B, Zhong Yichen, Zhuo Joe, Cichewicz Allie, Kadambi Ananth, Junqueira Daniela, Westley Tracy, Kisa Renata, Daamen Carolin, Augustin Matthias
University of California Los Angeles, Los Angeles, CA, USA.
Division of Dermatology, David Geffen Department of Medicine, University of California Los Angeles, 2001 Santa Monica Boulevard, Suite 1090, Santa Monica, CA, 90404, USA.
Dermatol Ther (Heidelb). 2023 Nov;13(11):2839-2857. doi: 10.1007/s13555-023-01034-7. Epub 2023 Oct 6.
Deucravacitinib, a newly approved oral medication for the treatment of patients with moderate to severe plaque psoriasis, demonstrated efficacy versus apremilast and placebo in two phase 3 randomized controlled trials (RCTs). A systematic review and network meta-analysis (NMA) indirectly compared deucravacitinib with other relevant systemic biologic/nonbiologic treatments.
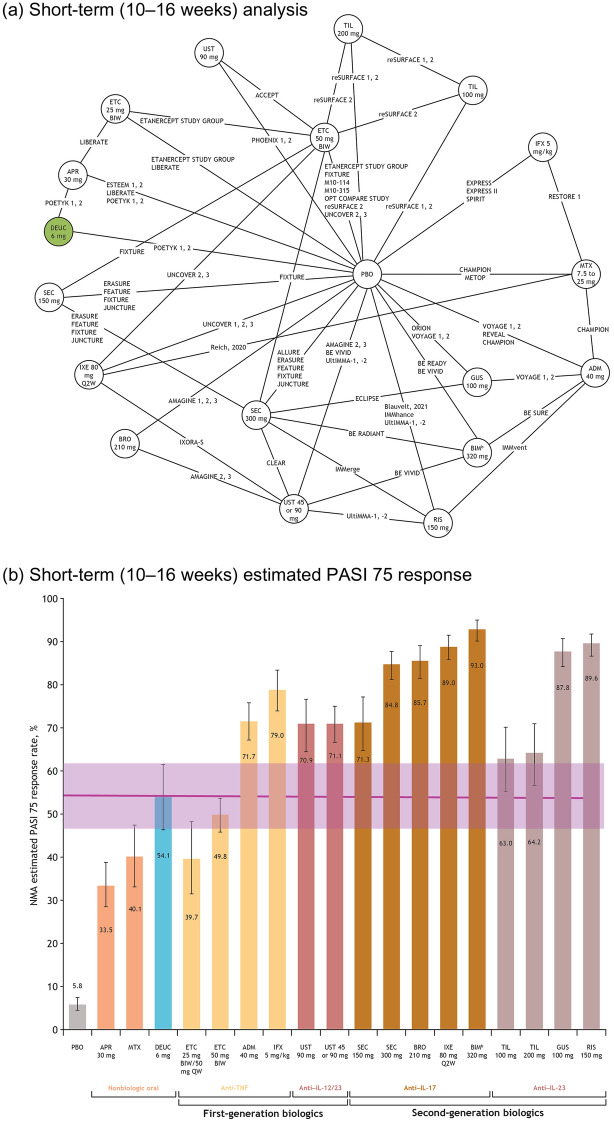
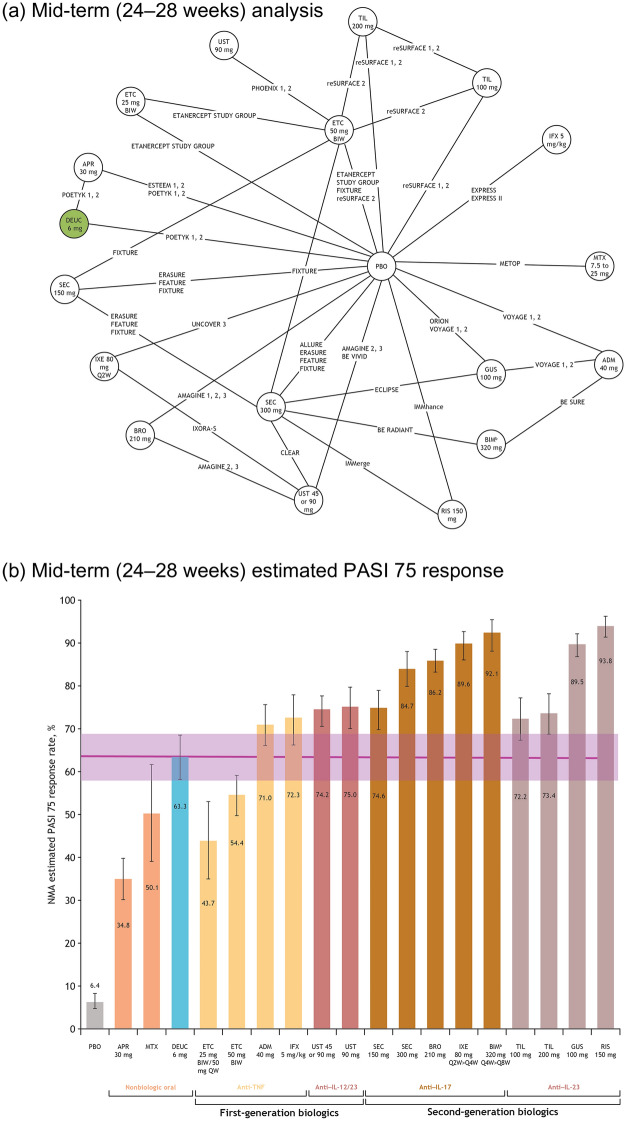
Online databases were searched for RCTs published through October 2021. Eligible studies were head-to-head comparisons between systemic therapies and/or placebo reporting 50%, 75%, 90%, or 100% improvement in Psoriasis Area and Severity Index (PASI) from baseline in adults with moderate to severe plaque psoriasis. Comparisons included tumor necrosis factor inhibitors, interleukin (IL)-17, IL-23, and IL 12/23 inhibitors, and systemic nonbiologics. A multinomial Bayesian NMA was used to derive estimates of the relative efficacy of deucravacitinib and other systemic therapies. Response probabilities for each treatment and corresponding 95% credible intervals (CrIs) for achieving a PASI response were calculated over short-, mid-, and long-term follow-up (weeks 10-16, 24-28, and 44-60).
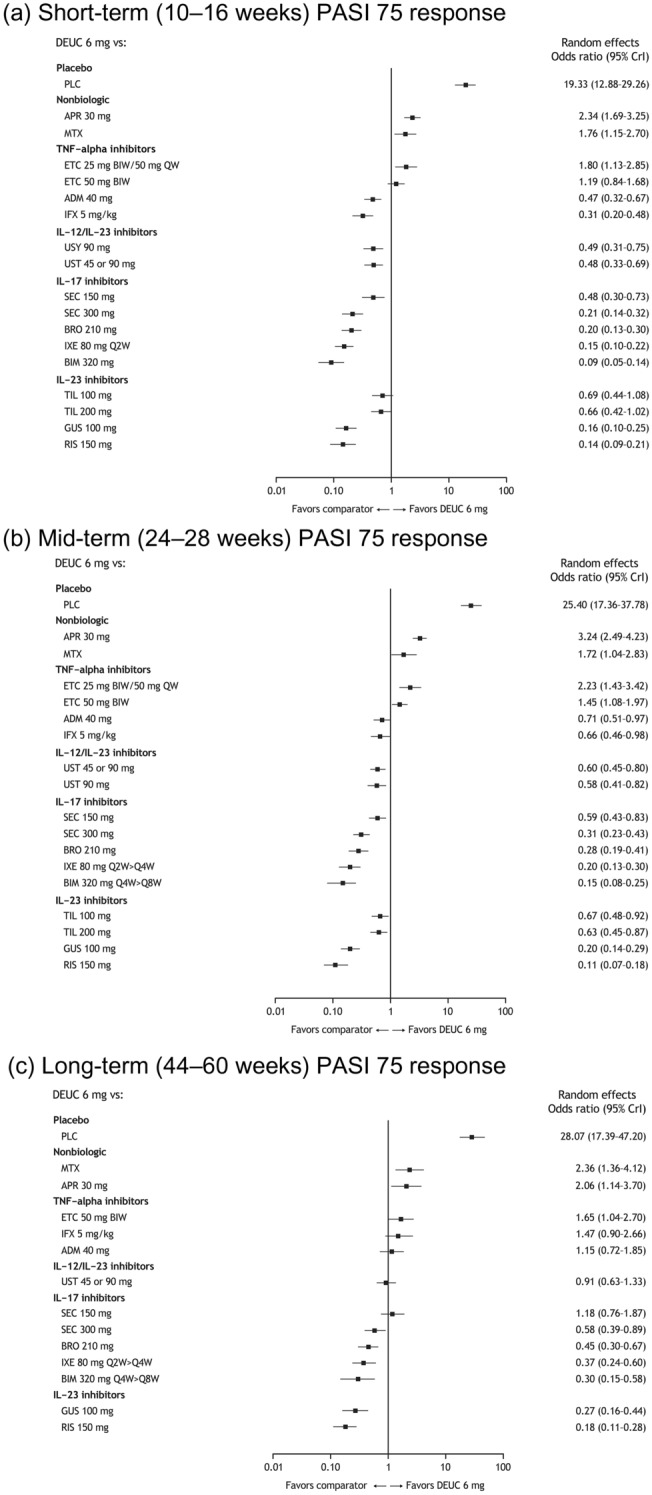
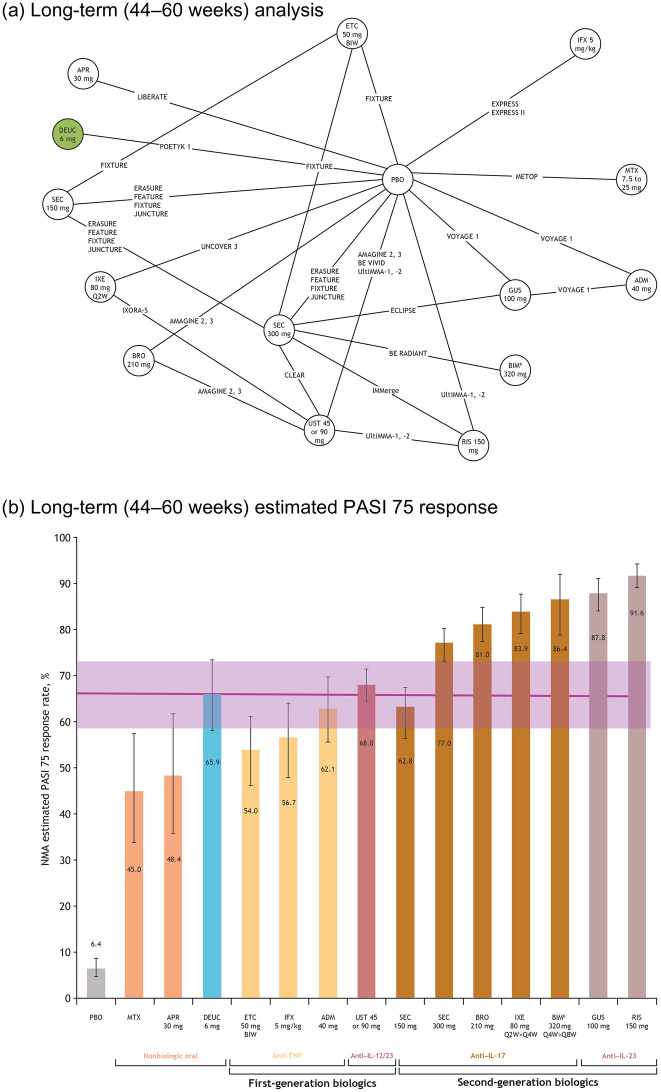
The NMA included 47 RCTs. Deucravacitinib showed the highest PASI 75 response rates among nonbiologic systemic therapies across time points. Deucravacitinib PASI 75 response rate (95% CrI) over short-term follow-up was 54.1% (46.5-61.6), within the range of first-generation biologics (etanercept, 39.7% [31.6-48.3]; infliximab, 79.0% [74.0-83.5]). At mid-term follow-up, deucravacitinib PASI 75 increased to 63.3% (58.0-68.4). At long-term follow-up, deucravacitinib PASI 75 was 65.9% (58.0-73.4), comparable to first-generation biologics adalimumab (62.8%; 55.3-69.6) and ustekinumab (68.0%; 64.6-71.5).
Patients receiving deucravacitinib were more likely to achieve PASI 75 response versus apremilast and methotrexate across all time points. The long-term PASI 75 response rate for deucravacitinib was similar to those of adalimumab and ustekinumab. The approval of deucravacitinib offers patients the choice of an oral therapy with long-term efficacy similar to that of some biologics.
德卡伐替尼是一种新批准的用于治疗中度至重度斑块状银屑病患者的口服药物,在两项3期随机对照试验(RCT)中显示出优于阿普米司特和安慰剂的疗效。一项系统评价和网状Meta分析(NMA)间接比较了德卡伐替尼与其他相关的全身生物制剂/非生物制剂治疗。
检索在线数据库,查找截至2021年10月发表的RCT。符合条件的研究为全身治疗和/或安慰剂之间的直接比较,报告中度至重度斑块状银屑病成人患者的银屑病面积和严重程度指数(PASI)从基线改善50%、75%、90%或100%。比较包括肿瘤坏死因子抑制剂、白细胞介素(IL)-17、IL-23和IL-12/23抑制剂,以及全身非生物制剂。使用多项贝叶斯NMA来估计德卡伐替尼和其他全身治疗的相对疗效。在短期、中期和长期随访(第10 - 16周、24 - 28周和44 - 60周)期间,计算每种治疗的反应概率以及达到PASI反应的相应95%可信区间(CrI)。
NMA纳入了47项RCT。在各时间点,德卡伐替尼在非生物全身治疗中显示出最高的PASI 75反应率。德卡伐替尼在短期随访中的PASI 75反应率(95% CrI)为54.1%(46.5 - 61.6),在第一代生物制剂的范围内(依那西普,39.7% [31.6 - 48.3];英夫利昔单抗,79.0% [74.0 - 83.5])。在中期随访时,德卡伐替尼的PASI 75增加到63.3%(58.0 - 68.4)。在长期随访时,德卡伐替尼的PASI 75为65.9%(58.0 - 73.4),与第一代生物制剂阿达木单抗(62.8%;55.3 - 69.6)和乌司奴单抗(68.0%;64.6 - 71.5)相当。
在所有时间点,接受德卡伐替尼治疗的患者比接受阿普米司特和甲氨蝶呤治疗的患者更有可能实现PASI 75反应。德卡伐替尼的长期PASI 75反应率与阿达木单抗和乌司奴单抗相似。德卡伐替尼的获批为患者提供了一种口服治疗选择,其长期疗效与某些生物制剂相似。