Clark Rebecca A, Portnoy Allison, Weerasuriya Chathika K, Sumner Tom, Bakker Roel, Harris Rebecca C, Rade Kirankumar, Mattoo Sanjay Kumar, Tumu Dheeraj, Menzies Nicolas A, White Richard G
TB Modelling Group and TB Centre, LSHTM.
Centre for the Mathematical Modelling of Infectious Diseases, LSHTM.
medRxiv. 2023 Sep 27:2023.09.27.23296211. doi: 10.1101/2023.09.27.23296211.
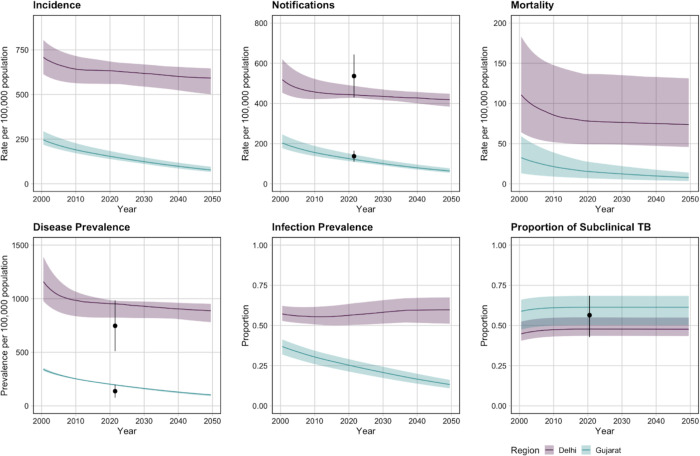
India has the largest tuberculosis burden globally, but this burden varies nationwide. All-age tuberculosis prevalence in 2021 ranged from 747/100,000 in Delhi to 137/100,000 in Gujarat. Previous modelling has demonstrated the benefits and costs of introducing novel tuberculosis vaccines in India overall. However, no studies have compared the potential impact of tuberculosis vaccines in regions within India with differing tuberculosis disease and infection prevalence. We used mathematical modelling to investigate how the health and economic impact of two potential tuberculosis vaccines, M72/AS01 and BCG-revaccination, could differ in Delhi and Gujarat under varying delivery strategies.
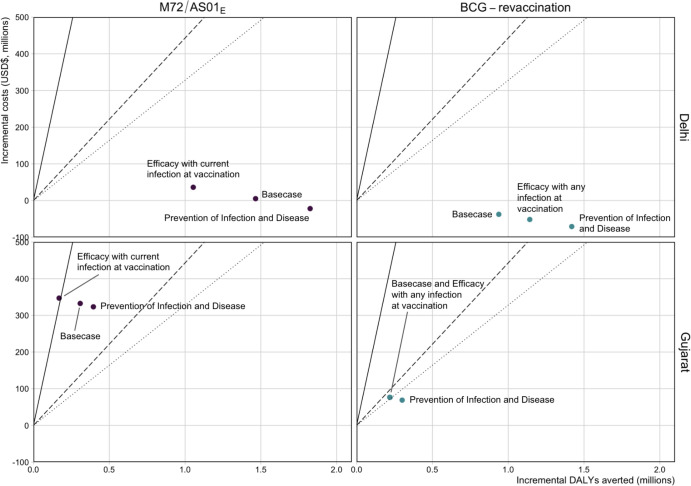
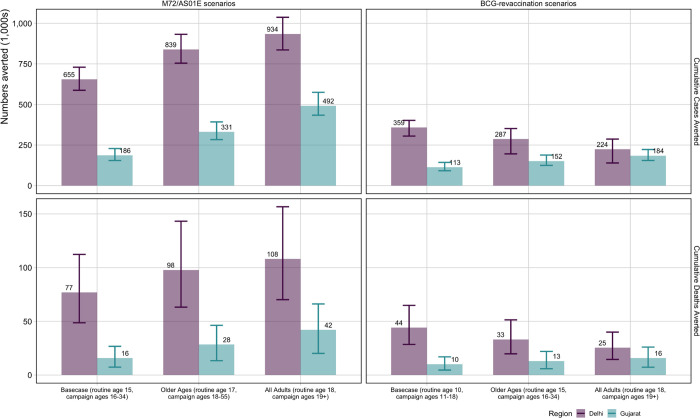
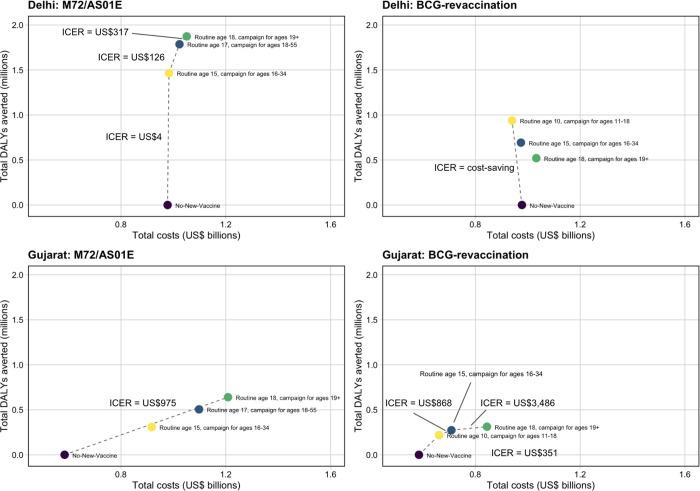
We applied a compartmental tuberculosis model separately for Delhi (higher disease and infection prevalence) and Gujarat (lower disease and infection prevalence), and projected epidemiological trends to 2050 assuming no new vaccine introduction. We simulated M72/AS01 and BCG-revaccination scenarios varying target ages and vaccine characteristics. We estimated cumulative cases, deaths, and disability-adjusted life years averted between 2025-2050 compared to the no-new-vaccine scenario and compared incremental cost-effectiveness ratios to three cost-effectiveness thresholds.
M72/AS01 averted a higher proportion of tuberculosis cases than BCG-revaccination in both regions (Delhi: 16.0% vs 8.3%, Gujarat: 8.5% vs 5.1%) and had higher vaccination costs (Delhi: USD$118 million vs USD$27 million, Gujarat: US$366 million vs US$97 million). M72/AS01 in Delhi could be cost-effective, or even cost-saving, for all modelled vaccine characteristics. M72/AS01 could be cost-effective in Gujarat, unless efficacy was assumed only for those with current infection at vaccination. BCG-revaccination could be cost-effective, or cost-saving, in both regions for all modelled vaccine scenarios.
M72/AS01 and BCG-revaccination could be impactful and cost-effective in Delhi and Gujarat. Differences in impact, costs, and cost-effectiveness between vaccines and regions, were determined partly by differences in disease and infection prevalence, and demography. Age-specific regional estimates of infection prevalence could help to inform delivery strategies for vaccines that may only be effective in people with a particular infection status. Evidence on the mechanism of effect of M72/AS01 and its effectiveness in uninfected individuals, which were important drivers of impact and cost-effectiveness, particularly in Gujarat, are also key to improve estimates of population-level impact.
印度是全球结核病负担最重的国家,但这种负担在全国范围内存在差异。2021年全年龄段结核病患病率从德里的747/10万到古吉拉特邦的137/10万不等。以往的模型研究已经证明了在印度总体上引入新型结核病疫苗的益处和成本。然而,尚无研究比较结核病疫苗在印度不同结核病疾病和感染患病率地区的潜在影响。我们使用数学模型来研究两种潜在的结核病疫苗M72/AS01和卡介苗复种在不同的接种策略下,对德里和古吉拉特邦的健康和经济影响可能会有怎样的不同。
我们分别为德里(疾病和感染患病率较高)和古吉拉特邦(疾病和感染患病率较低)应用了一个结核病 compartmental 模型,并假设不引入新疫苗,预测到2050年的流行病学趋势。我们模拟了M72/AS01和卡介苗复种的情景,改变目标年龄和疫苗特性。我们估计了与无新疫苗情景相比,2025年至2050年间避免的累计病例、死亡和伤残调整生命年,并将增量成本效益比与三个成本效益阈值进行了比较。
在两个地区,M72/AS01比卡介苗复种避免的结核病病例比例更高(德里:16.0%对8.3%,古吉拉特邦:8.5%对5.1%),且疫苗接种成本更高(德里:1.18亿美元对2700万美元,古吉拉特邦:3.66亿美元对9700万美元)。对于所有模拟的疫苗特性,德里的M72/AS01可能具有成本效益,甚至可能节省成本。M72/AS01在古吉拉特邦可能具有成本效益,除非仅假设对接种时现患感染的人群有效。对于所有模拟的疫苗情景,卡介苗复种在两个地区都可能具有成本效益或节省成本。
M72/AS01和卡介苗复种在德里和古吉拉特邦可能具有影响力且具有成本效益。疫苗和地区之间在影响、成本和成本效益方面的差异,部分是由疾病和感染患病率以及人口统计学的差异决定的。特定年龄的地区感染患病率估计有助于为可能仅对具有特定感染状态的人群有效的疫苗接种策略提供信息。关于M72/AS01的作用机制及其在未感染个体中的有效性的证据,是影响和成本效益的重要驱动因素,特别是在古吉拉特邦,也是改善人群水平影响估计的关键。