TB Modelling Group and TB Centre, London School of Hygiene and Tropical Medicine, Keppel Street, London, WC1E 7HT, UK.
Centre for the Mathematical Modelling of Infectious Diseases, London School of Hygiene and Tropical Medicine, London, UK.
BMC Med. 2023 Aug 4;21(1):288. doi: 10.1186/s12916-023-02992-7.
India had an estimated 2.9 million tuberculosis cases and 506 thousand deaths in 2021. Novel vaccines effective in adolescents and adults could reduce this burden. M72/AS01 and BCG-revaccination have recently completed phase IIb trials and estimates of their population-level impact are needed. We estimated the potential health and economic impact of M72/AS01 and BCG-revaccination in India and investigated the impact of variation in vaccine characteristics and delivery strategies.
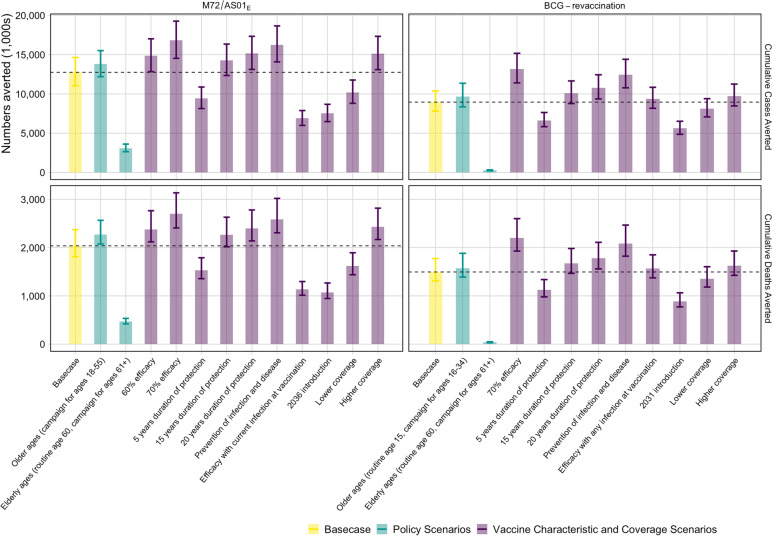
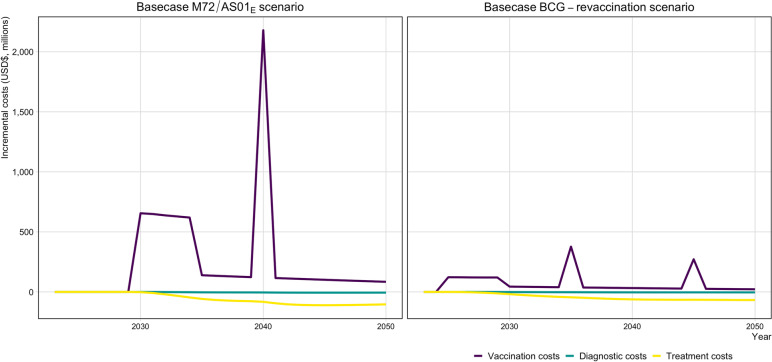
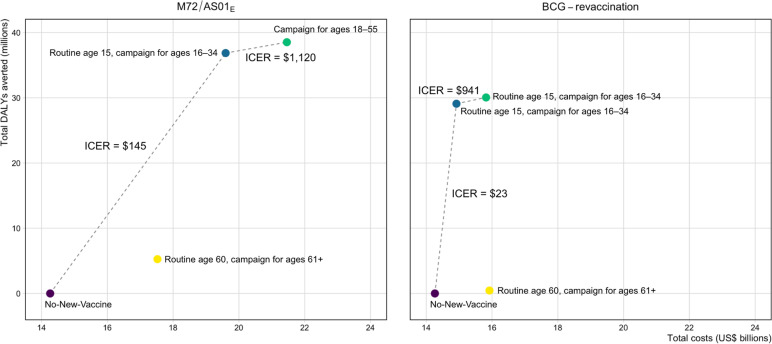
We developed an age-stratified compartmental tuberculosis transmission model for India calibrated to country-specific epidemiology. We projected baseline epidemiology to 2050 assuming no-new-vaccine introduction, and M72/AS01 and BCG-revaccination scenarios over 2025-2050 exploring uncertainty in product characteristics (vaccine efficacy, mechanism of effect, infection status required for vaccine efficacy, duration of protection) and implementation (achieved vaccine coverage and ages targeted). We estimated reductions in tuberculosis cases and deaths by each scenario compared to the no-new-vaccine baseline, as well as costs and cost-effectiveness from health-system and societal perspectives.
M72/AS01 scenarios were predicted to avert 40% more tuberculosis cases and deaths by 2050 compared to BCG-revaccination scenarios. Cost-effectiveness ratios for M72/AS01 vaccines were around seven times higher than BCG-revaccination, but nearly all scenarios were cost-effective. The estimated average incremental cost was US$190 million for M72/AS01 and US$23 million for BCG-revaccination per year. Sources of uncertainty included whether M72/AS01 was efficacious in uninfected individuals at vaccination, and if BCG-revaccination could prevent disease.
M72/AS01 and BCG-revaccination could be impactful and cost-effective in India. However, there is great uncertainty in impact, especially given the unknowns surrounding the mechanism of effect and infection status required for vaccine efficacy. Greater investment in vaccine development and delivery is needed to resolve these unknowns in vaccine product characteristics.
印度在 2021 年估计有 290 万例结核病病例和 50.6 万例死亡。新型疫苗在青少年和成年人中有效,可减轻这一负担。M72/AS01 和 BCG 再接种最近完成了 IIb 期试验,需要估计其对人群的影响。我们估计了 M72/AS01 和 BCG 再接种在印度的潜在健康和经济效益,并研究了疫苗特性和接种策略变化的影响。
我们为印度开发了一个按年龄分层的结核病传播模型,该模型根据该国特定的流行病学情况进行了校准。我们假设没有新疫苗引入,根据基线流行病学情况预测到 2050 年,然后根据 2025 年至 2050 年的 M72/AS01 和 BCG 再接种情况,探索产品特性(疫苗效力、作用机制、疫苗效力所需的感染状态、保护持续时间)和实施(实际疫苗覆盖率和目标年龄)的不确定性。我们根据每个方案与无新疫苗基线相比,估计了结核病病例和死亡人数的减少情况,以及从卫生系统和社会角度来看的成本和成本效益。
与 BCG 再接种方案相比,M72/AS01 方案预计到 2050 年可避免 40%的结核病病例和死亡。M72/AS01 疫苗的成本效益比约为 BCG 再接种的 7 倍,但几乎所有方案都具有成本效益。M72/AS01 每年的估计平均增量成本为 1.9 亿美元,BCG 再接种的成本为 2300 万美元。不确定性的来源包括 M72/AS01 在接种时对未感染者是否有效,以及 BCG 再接种是否能预防疾病。
M72/AS01 和 BCG 再接种在印度可能具有影响力和成本效益。然而,影响方面存在很大的不确定性,特别是考虑到疫苗效力所需的作用机制和感染状态的不确定性。需要增加疫苗开发和接种方面的投资,以解决疫苗产品特性方面的这些不确定性。