Service of Geriatric Medicine and Geriatric Rehabilitation, Lausanne University Hospital and University of Lausanne, Chemin de Mont Paisible 16, Lausanne, CH-1011, Switzerland.
Department of Geriatrics, Rehabilitation and Palliative Care, Neuchâtel Hospital Network, Rue du Chasseral 20, La Chaux-de-Fonds, CH-2300, Switzerland.
BMC Geriatr. 2023 Oct 10;23(1):642. doi: 10.1186/s12877-023-04321-2.
Comprehensive geriatric assessment (CGA) is difficult to perform in the emergency department (ED) environment and performance of screening tools in identifying vulnerable older ED patients who are best candidates for a geriatric consultation remain questionable.
To determine the characteristics of older patients referred for a geriatric consultation by ED staff and to investigate these patients' subsequent healthcare utilization.
Secondary analysis of data previously collected for a prospective observational study of patients aged 75 + years visiting the ED of an academic hospital in Switzerland over four months (Michalski-Monnerat et al., J Am Geriatr Soc 68(12):2914-20, 2020). Socio-demographic, health, functional (basic activities of daily living; BADL), cognitive, and affective status data were collected at admission by a research nurse using a standardized brief geriatric assessment. Information on geriatric consultations, hospitalization, discharge destination, and 30-day readmission were retrieved from hospital database. Bivariable and multivariable analyses were performed using this data set collected previously.
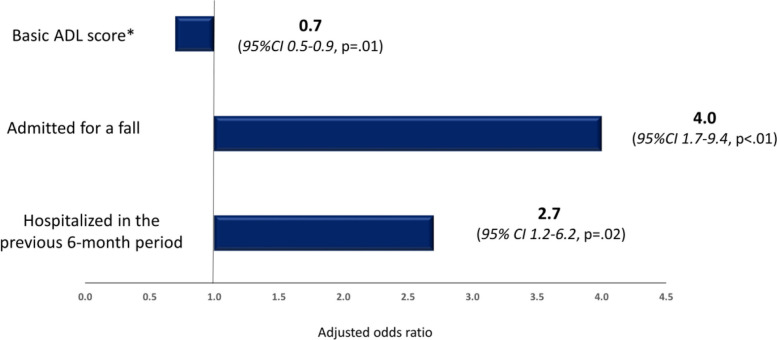
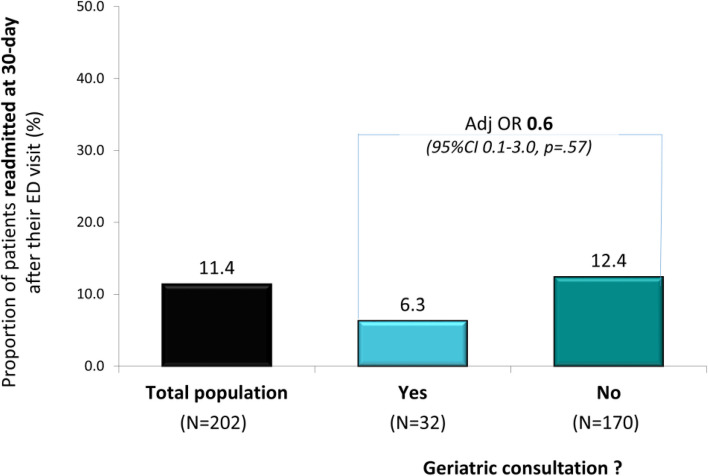
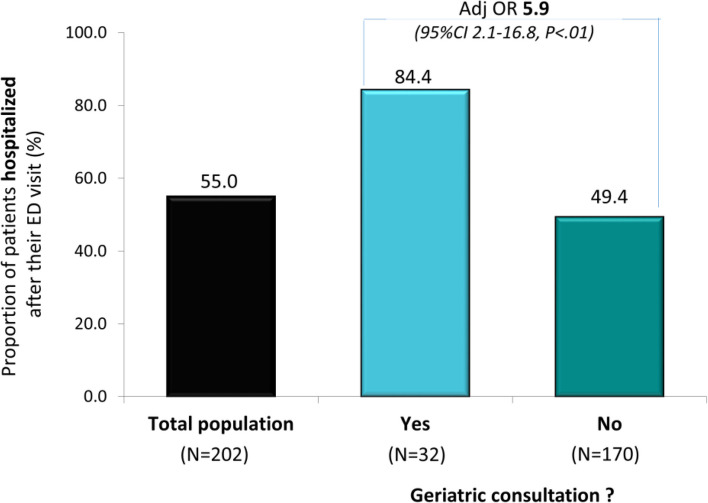
Thirty-two (15.8%) of the 202 enrolled patients were referred for a geriatric consultation. Compared to the others, they were older (84.9 ± 5.4 vs 82.9 ± 5.4 years, p = .03), more impaired in BADL (4.8 ± 1.6 vs 5.5 ± 1.0, p = .01), with more comorbid conditions (5.3 ± 1.5 vs 4.5 ± 1.9, p = .03), more frequently admitted after a fall (43.7% vs 19.4%, p = .01), and hospitalized over the previous 6-month period (53.1% vs 30.6%, p = .02). Multivariable analyses that adjusted for variables significantly associated with outcomes in bivariable analysis found that being admitted after a fall (AdjOR 4.0, 95%CI 1.7-9.4, p < .01) and previously hospitalized (AdjOR 2.7, 95% CI 1.2-6.2, p = .02) remained associated with increased odds of consultation, whereas the inverse association with BADL performance remained (AdjOR 0.7, 95%CI 0.5-0.9, p = .01). Patients referred for geriatric consultation had higher odds of hospitalization (84.4% vs 49.4%; AdjOR 5.9, 95%CI 2.1-16.8, p < .01), but similar odds of home discharge when admitted, and of 30-day readmission.
About one in six older ED patients were referred for a geriatric consultation who appeared to be those most vulnerable, as suggested by their increased hospitalization rate. Alternative strategies are needed to enhance access to geriatric consultation in the ED.
综合老年评估(CGA)在急诊科(ED)环境中难以进行,而筛查工具在识别最适合老年咨询的脆弱老年 ED 患者方面的表现仍存在疑问。
确定由 ED 工作人员转介接受老年咨询的老年患者的特征,并调查这些患者随后的医疗保健利用情况。
对先前在瑞士一家学术医院 ED 就诊的 75 岁及以上患者进行前瞻性观察研究中收集的数据进行二次分析(Michalski-Monnerat 等人,J Am Geriatr Soc 68(12):2914-20, 2020)。入院时,研究护士使用标准化的简要老年评估收集社会人口统计学、健康、功能(基本日常生活活动;BADL)、认知和情感状况数据。从医院数据库中检索有关老年咨询、住院、出院去向和 30 天再入院的信息。使用之前收集的数据进行单变量和多变量分析。
在纳入的 202 名患者中,有 32 名(15.8%)被转介接受老年咨询。与其他患者相比,他们年龄更大(84.9±5.4 岁 vs 82.9±5.4 岁,p=0.03),BADL 功能更差(4.8±1.6 vs 5.5±1.0,p=0.01),合并症更多(5.3±1.5 岁 vs 4.5±1.9 岁,p=0.03),跌倒后入院的频率更高(43.7% vs 19.4%,p=0.01),且在过去 6 个月内住院治疗(53.1% vs 30.6%,p=0.02)。对单变量分析中与结果显著相关的变量进行多变量分析发现,跌倒后入院(调整后的优势比 [AdjOR] 4.0,95%置信区间 [CI] 1.7-9.4,p<0.01)和之前住院(AdjOR 2.7,95%CI 1.2-6.2,p=0.02)与咨询的可能性增加相关,而与 BADL 表现的负相关仍然存在(AdjOR 0.7,95%CI 0.5-0.9,p=0.01)。接受老年咨询的患者住院的可能性更高(84.4% vs 49.4%;AdjOR 5.9,95%CI 2.1-16.8,p<0.01),但入院时和 30 天内的家庭出院可能性以及再入院率相似。
约六分之一的老年 ED 患者被转介接受老年咨询,他们似乎是最脆弱的患者,这表明他们的住院率更高。需要采取替代策略来增加 ED 中接受老年咨询的机会。