Université Paris-Est Créteil, INSERM, IMRB, Créteil, France; AP-HP, Henri-Mondor Hospital, Public Health Department & Clinical Research Unit (URC Mondor), Créteil, France; Institut Universitaire de Cancérologie (IUC), AP-HP, Sorbonne Université, Paris, France; Department of Medical Oncology, AP-HP, Tenon Hospital, Paris, France.
Université Paris-Est Créteil, INSERM, IMRB, Créteil, France; AP-HP, Henri-Mondor Hospital, Public Health Department & Clinical Research Unit (URC Mondor), Créteil, France.
ESMO Open. 2023 Oct;8(5):101831. doi: 10.1016/j.esmoop.2023.101831. Epub 2023 Oct 11.
In older patients, comorbidities competed with cancer for mortality risk. We assessed the prognostic value of comorbidities in older patients with cancer.
We analysed all patients >70 years of age with colorectal, breast, prostate, or lung cancer included in the prospective ELCAPA cohort. The Cumulative Illness Rating Scale-Geriatrics (CIRS-G) score was used to assess comorbidities. The primary endpoint was overall survival (OS) at 3, 12, and 36 months. The adjusted difference in the restricted mean survival time (RMST) was used to assess the strength of the relationship between comorbidities and survival.
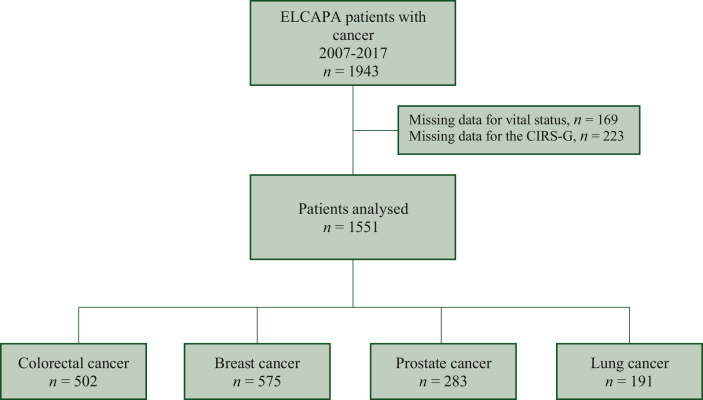
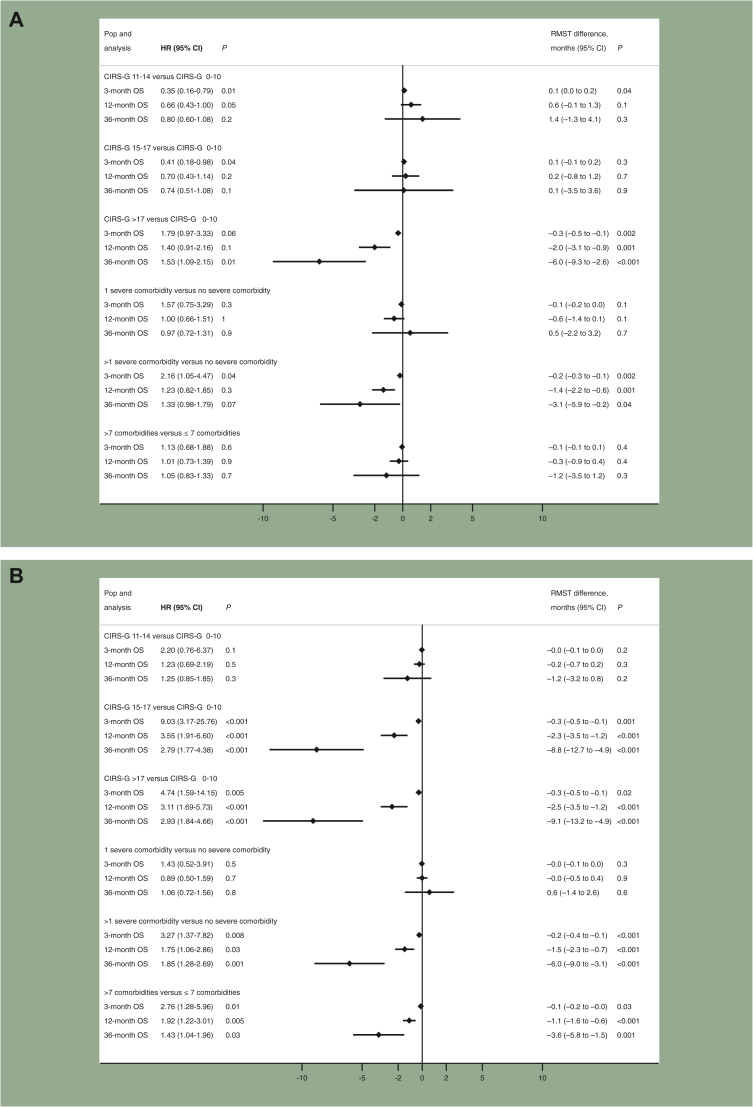
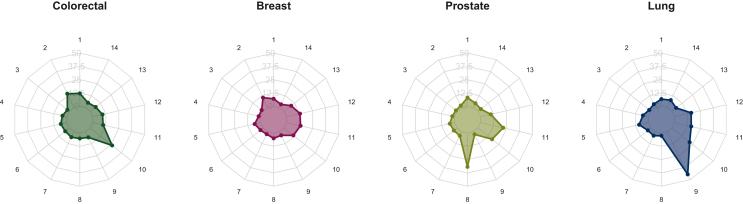
Of the 1551 patients included (median age 82 years; interquartile range 78-86 years), 502 (32%), 575 (38%), 283 (18%), and 191 (12%) had colorectal, breast, prostate, and lung cancer, respectively, and 50% had metastatic disease. Hypertension, kidney failure, and cognitive impairment were the most common comorbidities (67%, 38%, and 29% of the patients, respectively). A CIRS-G score >17, two or more severe comorbidities, more than seven comorbidities, heart failure, and cognitive impairment were independently associated with shorter OS. The greatest effect size was observed for CIRS-G >17 (versus CIRS-G <11): at 36 months, the adjusted differences in the RMST (95% confidence interval) were -6.0 months (-9.3 to -2.6 months) for colorectal cancer, -9.1 months (-13.2 to -4.9 months) for breast cancer, -8.3 months (-12.8 to -3.9 months) for prostate cancer, and -5.5 months (-9.9 to -1.1 months) for lung cancer (P < 0.05 for all).
Comorbidities' type, number, and severity were independently associated with shorter OS. A 17-point cut-off over 56 for the total CIRS-G score could be considered in clinical practice.
在老年患者中,合并症与癌症共同影响死亡风险。我们评估了合并症在老年癌症患者中的预后价值。
我们分析了纳入前瞻性 ELCAPA 队列的所有年龄>70 岁的结直肠癌、乳腺癌、前列腺癌或肺癌患者。使用累积疾病评分-老年(CIRS-G)量表评估合并症。主要终点是 3、12 和 36 个月的总生存(OS)。受限平均生存时间(RMST)的调整差异用于评估合并症与生存之间的关系强度。
在纳入的 1551 例患者中(中位年龄 82 岁;四分位距 78-86 岁),502 例(32%)、575 例(38%)、283 例(18%)和 191 例(12%)分别患有结直肠癌、乳腺癌、前列腺癌和肺癌,50%的患者有转移病灶。高血压、肾衰竭和认知障碍是最常见的合并症(分别占患者的 67%、38%和 29%)。CIRS-G 评分>17、两种或两种以上严重合并症、七种以上合并症、心力衰竭和认知障碍与较短的 OS 独立相关。最大的效应大小观察到 CIRS-G>17(与 CIRS-G<11 相比):在 36 个月时,RMST(95%置信区间)的调整差异为结直肠癌为-6.0 个月(-9.3 至-2.6 个月)、乳腺癌为-9.1 个月(-13.2 至-4.9 个月)、前列腺癌为-8.3 个月(-12.8 至-3.9 个月),肺癌为-5.5 个月(-9.9 至-1.1 个月)(均 P<0.05)。
合并症的类型、数量和严重程度与较短的 OS 独立相关。在临床实践中,可以考虑将 CIRS-G 总评分的 56 分作为 17 分的截断值。