Department of Pharmacy, The University of Tokyo Hospital, 7-3-1 Hongo, Bunkyo-Ku, Tokyo, 113-8655, Japan.
The Education Center for Clinical Pharmacy, Graduate School of Pharmaceutical Sciences, The University of Tokyo, 7-3-1 Hongo, Bunkyo-Ku, Tokyo, 113-8655, Japan.
BMC Cancer. 2023 Oct 13;23(1):979. doi: 10.1186/s12885-023-11469-y.
Weekly paclitaxel + ramucirumab (wPTX + RAM) therapy is recommended as the standard second-line chemotherapy regimen for unresectable advanced/recurrent gastric cancer (GC) or esophagogastric junction cancer. Recent subgroup analysis of the RAINBOW trial revealed a higher frequency of severe neutropenia due to wPTX + RAM in Japanese compared to Western patients. However, no risk factors for severe neutropenia have been identified.
This retrospective observational study included patients with advanced/unresectable gastric or esophagogastric junction cancer who received wPTX + RAM after failure to respond to platinum and fluoropyrimidine doublet chemotherapy between June 2015 and April 2020. We conducted multivariable logistic regression analyses to identify the risk factors associated with grade 4 neutropenia and febrile neutropenia (FN). In addition, we investigated the relationship between the number of risk factors and overall survival (OS) and progression-free survival (PFS).
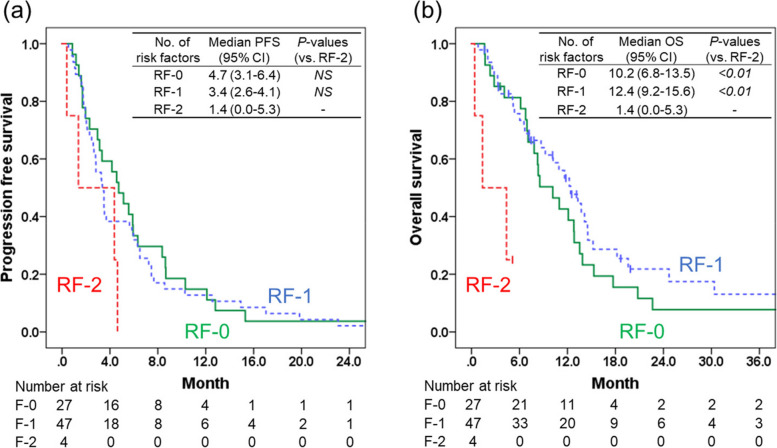
Among 66 patients who met the inclusion criteria, grade 4 neutropenia and FN occurred in 21 (31.8%) and 12 (18.2%) patients, respectively. Prior treatment with oxaliplatin-containing regimens was identified as an independent risk factor for developing grade 4 neutropenia (odds ratio (OR) 20.034, 95% confidence interval (95% CI) 3.216-124.807, P = 0.001). Total bilirubin of > 1.5 mg/dL (OR 31.316, 95% CI 2.052-477.843, P = 0.013) and prior treatment with oxaliplatin-containing regimen (OR 12.502, 95% CI 1.141-137.022, P = 0.039) were identified as independent risk factors for developing FN. Next, we classified patients with 0, 1, 2 risk factor(s) as RF-0, RF-1, and RF-2 subgroups, respectively, and compared the PFS and OS among the three subgroups. PFS was not significantly different among the three subgroups, whereas OS was significantly shorter in the RF-2 subgroup (median 1.4 month, 95% CI 0.0-5.3 month) than in the RF-0 subgroup (median 10.2 month, 95% CI 6.8-13.5 month, P < 0.01 vs RF-2) and RF-1 subgroup (median 13.3 month, 95% CI 10.9-15.7 month, P < 0.01 vs RF-2).
Careful monitoring for grade 4 neutropenia and FN is needed for patients receiving wPTX + RAM therapy who have a history of treatment with oxaliplatin-containing regimens and higher total bilirubin levels.
每周紫杉醇 + 雷莫芦单抗(wPTX + RAM)治疗被推荐为不可切除的晚期/复发性胃(GC)或食管胃结合部癌的标准二线化疗方案。RAINBOW 试验的最近亚组分析显示,与西方患者相比,日本患者接受 wPTX + RAM 治疗后中性粒细胞减少症的严重程度更高。然而,尚未确定导致严重中性粒细胞减少症的危险因素。
本回顾性观察性研究纳入了自 2015 年 6 月至 2020 年 4 月期间接受铂类和氟嘧啶双联化疗治疗失败的晚期/不可切除胃或食管胃结合部癌患者,他们接受了 wPTX + RAM 治疗。我们进行了多变量逻辑回归分析,以确定与 4 级中性粒细胞减少症和发热性中性粒细胞减少症(FN)相关的危险因素。此外,我们研究了危险因素数量与总生存期(OS)和无进展生存期(PFS)之间的关系。
在符合纳入标准的 66 名患者中,分别有 21 名(31.8%)和 12 名(18.2%)患者发生 4 级中性粒细胞减少症和 FN。含奥沙利铂方案的既往治疗被确定为发生 4 级中性粒细胞减少症的独立危险因素(比值比(OR)20.034,95%置信区间(95%CI)3.216-124.807,P = 0.001)。总胆红素>1.5 mg/dL(OR 31.316,95%CI 2.052-477.843,P = 0.013)和含奥沙利铂方案的既往治疗(OR 12.502,95%CI 1.141-137.022,P = 0.039)被确定为发生 FN 的独立危险因素。接下来,我们将 0、1、2 个危险因素的患者分别分类为 RF-0、RF-1 和 RF-2 亚组,并比较了三个亚组之间的 PFS 和 OS。三个亚组之间的 PFS 无显著差异,而 OS 在 RF-2 亚组(中位 1.4 个月,95%CI 0.0-5.3 个月)显著短于 RF-0 亚组(中位 10.2 个月,95%CI 6.8-13.5 个月,P < 0.01 与 RF-2)和 RF-1 亚组(中位 13.3 个月,95%CI 10.9-15.7 个月,P < 0.01 与 RF-2)。
对于接受 wPTX + RAM 治疗且有含奥沙利铂方案治疗史和较高总胆红素水平的患者,需要密切监测 4 级中性粒细胞减少症和 FN。