Centre for Cardiovascular Science, University of Edinburgh Division of Clinical and Surgical Sciences, Edinburgh, UK
Thrombosis Research Institute, London, UK.
BMJ Open. 2022 Jan 7;12(1):e049933. doi: 10.1136/bmjopen-2021-049933.
In patients with newly diagnosed atrial fibrillation (AF), do baseline risk factors and stroke prevention strategies account for the geographically diverse outcomes.
Global Anticoagulant Registry in the FIELD-Atrial Fibrillation is a prospective multinational non-interventional registry of patients with newly diagnosed AF (n=52 018 patients).
Investigator sites (n=1317) were representative of the care settings/locations in each of the 35 participating countries. Treatment decisions were all determined by the local responsible clinicians.
The patients (18 years and over) with newly diagnosed AF had at least 1 investigator-determined stroke risk factor and patients were not required to meet specific thresholds of risk score for anticoagulant treatment.
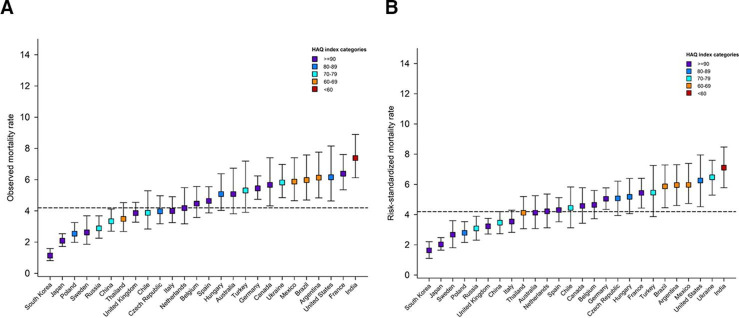
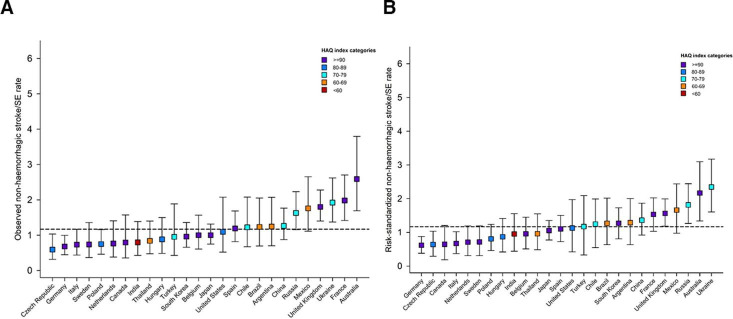
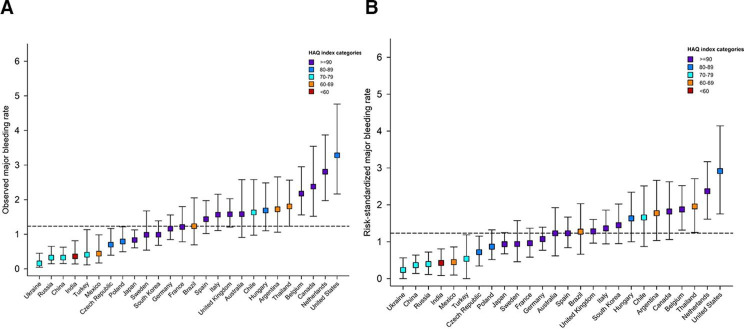
Observed 1-year event rates and risk-standardised rates were derived.
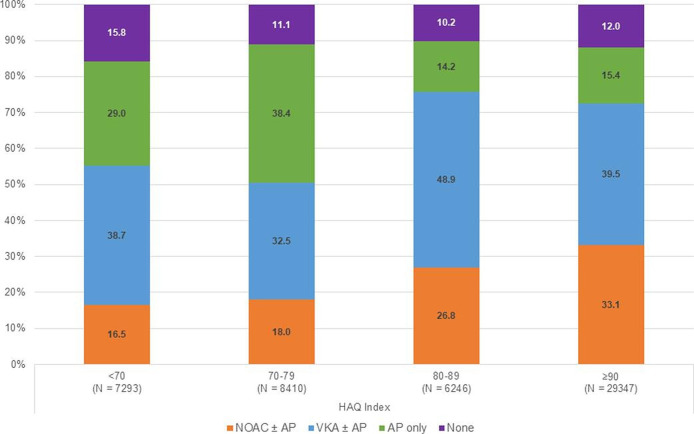
Rates of death, non-haemorrhagic stroke/systemic embolism and major bleeding varied more than three-to-four fold across countries even after adjustment for baseline factors and antithrombotic treatments. Rates of anticoagulation and antithrombotic treatment varied widely. Patients from countries with the highest rates of cardiovascular mortality and stroke were among the least likely to receive oral anticoagulants. Beyond anticoagulant treatment, variations in the treatment of comorbidities and lifestyle factors may have contributed to the variations in outcomes. Countries with the lowest healthcare Access and Quality indices (India, Ukraine, Argentina, Brazil) had the highest risk-standardised mortality.
The variability in outcomes across countries for patients with newly diagnosed AF is not accounted for by baseline characteristics and antithrombotic treatments. Residual mortality rates were correlated with Healthcare Access and Quality indices. The findings suggest the management of patients with AF needs to not only address guideline indicated and sustained anticoagulation, but also the treatment of comorbidities and lifestyle factors.
NCT01090362.
在新发心房颤动(AF)患者中,基线风险因素和卒中预防策略是否能解释地域差异的结局。
全球抗凝注册研究-心房颤动(Global Anticoagulant Registry in the FIELD-Atrial Fibrillation)是一项前瞻性、多国、非干预性、新发 AF 患者注册研究(n=52018 例患者)。
研究者场所(n=1317)代表了 35 个参与国家中每个国家的治疗环境/地点。所有治疗决策均由当地负责的临床医生决定。
新诊断为 AF 的患者(18 岁及以上)至少有 1 项研究者确定的卒中风险因素,且患者无需满足抗凝治疗的特定风险评分阈值。
得出观察到的 1 年事件发生率和风险标准化发生率。
即使在调整了基线因素和抗血栓治疗后,各国之间的死亡率、非出血性卒中和全身性栓塞以及大出血发生率仍相差 3 至 4 倍以上。抗凝和抗血栓治疗的比率差异很大。心血管死亡率和卒中发生率最高的国家的患者最不可能接受口服抗凝剂治疗。除了抗凝治疗之外,治疗合并症和生活方式因素的差异也可能导致结局的差异。医疗保健获取和质量指数最低的国家(印度、乌克兰、阿根廷、巴西)的风险标准化死亡率最高。
新发 AF 患者的结局在各国之间存在差异,这不能用基线特征和抗血栓治疗来解释。残余死亡率与医疗保健获取和质量指数相关。这些发现表明,AF 患者的管理不仅需要解决指南建议的和持续的抗凝治疗,还需要治疗合并症和生活方式因素。
NCT01090362。