University Hospital Würzburg, Department of Anaesthesiology, Intensive Care, Emergency and Pain Medicine, Oberdürrbacher Str. 6, 97080, Würzburg, Germany.
Department of Cardiac Anesthesiology and Intensive Care Medicine, Charité Berlin, Berlin, Germany.
Crit Care. 2023 Oct 18;27(1):399. doi: 10.1186/s13054-023-04663-8.
Based on low-quality evidence, current nutrition guidelines recommend the delivery of high-dose protein in critically ill patients. The EFFORT Protein trial showed that higher protein dose is not associated with improved outcomes, whereas the effects in critically ill patients who developed acute kidney injury (AKI) need further evaluation. The overall aim is to evaluate the effects of high-dose protein in critically ill patients who developed different stages of AKI.
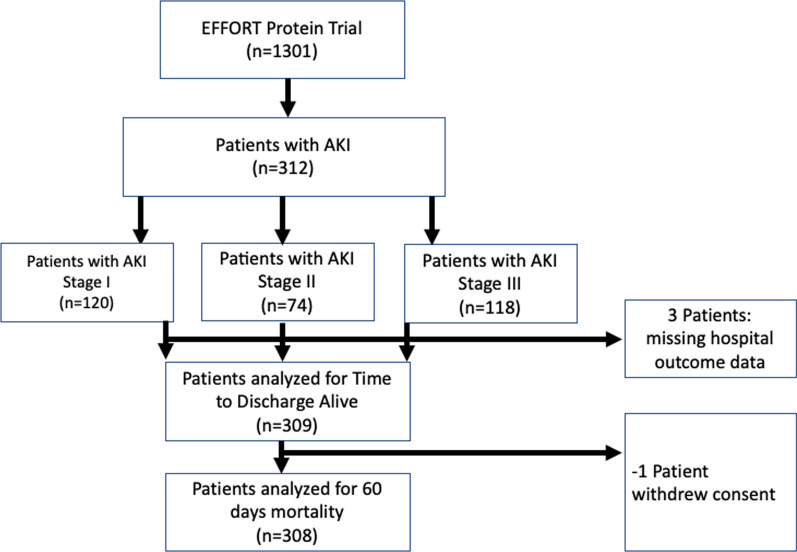
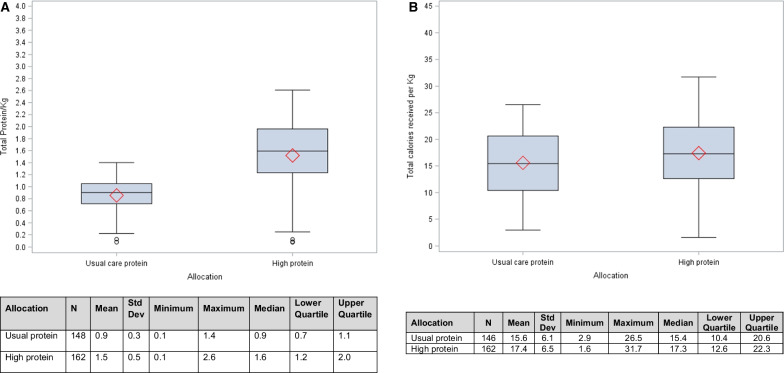
In this post hoc analysis of the EFFORT Protein trial, we investigated the effect of high versus usual protein dose (≥ 2.2 vs. ≤ 1.2 g/kg body weight/day) on time-to-discharge alive from the hospital (TTDA) and 60-day mortality and in different subgroups in critically ill patients with AKI as defined by the Kidney Disease Improving Global Outcomes (KDIGO) criteria within 7 days of ICU admission. The associations of protein dose with incidence and duration of kidney replacement therapy (KRT) were also investigated.
Of the 1329 randomized patients, 312 developed AKI and were included in this analysis (163 in the high and 149 in the usual protein dose group). High protein was associated with a slower time-to-discharge alive from the hospital (TTDA) (hazard ratio 0.5, 95% CI 0.4-0.8) and higher 60-day mortality (relative risk 1.4 (95% CI 1.1-1.8). Effect modification was not statistically significant for any subgroup, and no subgroups suggested a beneficial effect of higher protein, although the harmful effect of higher protein target appeared to disappear in patients who received kidney replacement therapy (KRT). Protein dose was not significantly associated with the incidence of AKI and KRT or duration of KRT.
In critically ill patients with AKI, high protein may be associated with worse outcomes in all AKI stages. Recommendation of higher protein dosing in AKI patients should be carefully re-evaluated to avoid potential harmful effects especially in patients who were not treated with KRT.
This study is registered at ClinicalTrials.gov (NCT03160547) on May 17th 2017.
基于低质量证据,目前的营养指南建议对重症患者给予高剂量蛋白质。EFFORT Protein 试验表明,较高的蛋白质剂量与改善结局无关,而在发生急性肾损伤(AKI)的重症患者中的作用需要进一步评估。总体目标是评估高剂量蛋白质对发生不同阶段 AKI 的重症患者的影响。
在 EFFORT Protein 试验的这项事后分析中,我们研究了高剂量与常规剂量(≥2.2 与≤1.2g/kg 体重/天)对 ICU 入院后 7 天内发生 AKI (根据 KDIGO 标准定义)的重症患者从医院出院时间(TTDA)和 60 天死亡率的影响,以及不同亚组的影响。还研究了蛋白质剂量与肾脏替代治疗(KRT)的发生率和持续时间的关系。
在 1329 名随机患者中,312 名发生 AKI 并纳入本分析(高剂量组 163 例,常规剂量组 149 例)。高蛋白质与出院时间较慢相关(危险比 0.5,95%CI 0.4-0.8),60 天死亡率较高(相对风险 1.4(95%CI 1.1-1.8)。任何亚组的效应修饰均无统计学意义,没有亚组表明高蛋白质有有益作用,尽管在接受肾脏替代治疗(KRT)的患者中,高蛋白质目标的有害作用似乎消失。蛋白质剂量与 AKI 和 KRT 的发生率或 KRT 的持续时间无显著相关性。
在发生 AKI 的重症患者中,高蛋白质可能与所有 AKI 阶段的不良结局相关。建议对 AKI 患者给予更高的蛋白质剂量应谨慎重新评估,以避免潜在的有害影响,特别是在未接受 KRT 治疗的患者中。
本研究于 2017 年 5 月 17 日在 ClinicalTrials.gov(NCT03160547)注册。