Xiong Jianzhu, Chen Kangkang, Huang Wen, Huang Mingang, Cao Feiyan, Wang Yiwen, Chen Qifeng
Department of Public Health, Shaoxing Seventh People's Hospital, Shaoxing, China.
Department of Non-communicable Diseases Control and Prevention, Shaoxing Center for Disease Control and Prevention, Shaoxing, China.
Front Oncol. 2023 Oct 6;13:1249353. doi: 10.3389/fonc.2023.1249353. eCollection 2023.
BACKGROUND & AIMS: Evidence regarding the prevalence of pre-treatment sarcopenia and its impact on survival in patients with hematological malignancies (HM) varies across studies. We conducted a systematic review and meta-analysis to summarize this discrepancy.
PubMed, Embase and Cochrane library were systematically searched for relevant studies. Outcomes assessed were: prevalence of pre-treatment sarcopenia, overall survival (OS), progression-free survival (PFS) and complete response (CR). Weighted mean proportion, odds ratios (ORs) and hazard ratios (HRs) were estimated using a fixed-effects and a random-effects model.
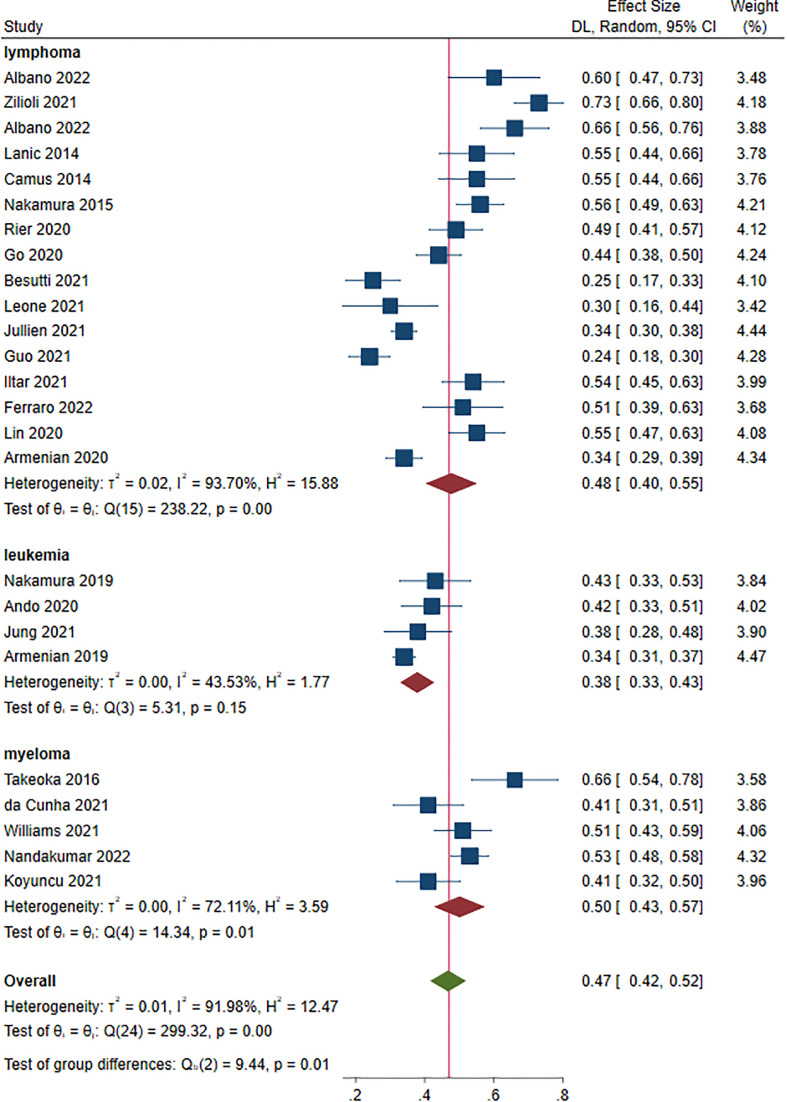
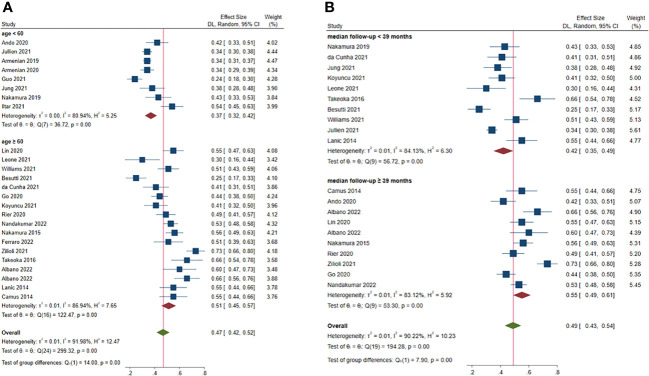
A total of 27 retrospective cohort studies involving 4,991 patients were included in this study. The prevalence of pre-treatment sarcopenia was 37.0% (95% CI: 32.0%-42.0%) in HM patients <60 years and 51.0% (95% CI: 45.0%-57.0%) in≥60 years. Patients with leukemia had the lowest prevalence, compared with those with other HM (38.0%; 95% CI: 33.0%-43.0%; = 0.010). The presence of sarcopenia was independently associated with poor OS (HR = 1.57, 95% CI = 1.41-1.75) and PFS (HR = 1.50, 95% CI = 1.22-1.83) throughout treatment period, which may be partially attributed to decreased CR (OR = 0.54, 95% CI = 0.41-0.72), particularly for BMI ≥ 25 ( = 0.020) and males ( = 0.020).
Sarcopenia is highly prevalent in patients with HM and an adverse prognostic factor for both survival and treatment efficacy. HM and sarcopenia can aggravate each other. We suggest that in future clinical work, incorporating sarcopenia into risk scores will contribute to guide patient stratification and therapeutic strategy, particularly for the elderly.
https://www.crd.york.ac.uk/prospero/, identifier (CRD42023392550).
关于血液系统恶性肿瘤(HM)患者治疗前肌肉减少症的患病率及其对生存影响的证据在不同研究中存在差异。我们进行了一项系统评价和荟萃分析以总结这种差异。
系统检索PubMed、Embase和Cochrane图书馆中的相关研究。评估的结局包括:治疗前肌肉减少症的患病率、总生存期(OS)、无进展生存期(PFS)和完全缓解(CR)。使用固定效应模型和随机效应模型估计加权平均比例、比值比(OR)和风险比(HR)。
本研究共纳入27项涉及4991例患者的回顾性队列研究。年龄<60岁的HM患者治疗前肌肉减少症的患病率为37.0%(95%CI:32.0%-42.0%),≥60岁患者为51.0%(95%CI:45.0%-57.0%)。与其他HM患者相比,白血病患者的患病率最低(38.0%;95%CI:33.0%-43.0%;P = 0.010)。在整个治疗期间,肌肉减少症的存在与较差的OS(HR = 1.57,95%CI = 1.41-1.75)和PFS(HR = 1.50,95%CI = 1.22-1.83)独立相关,这可能部分归因于CR降低(OR = 0.54,95%CI = 0.41-0.72),特别是对于BMI≥25(P = 0.020)和男性(P = 0.020)。
肌肉减少症在HM患者中高度流行,是生存和治疗疗效的不良预后因素。HM和肌肉减少症可相互加重。我们建议在未来的临床工作中,将肌肉减少症纳入风险评分将有助于指导患者分层和治疗策略,特别是对于老年人。