Department of Epidemiology and Biostatistics, Memorial Sloan Kettering Cancer Center, New York, NY 10017, USA
Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
BMJ. 2023 Oct 25;383:e075512. doi: 10.1136/bmj-2023-075512.
To estimate the association between oncologists' receipt of payments from the pharmaceutical industry and delivery of non-recommended or low value interventions among their patients.
Cohort study.
Fee-for-service Medicare claims.
Medicare beneficiaries with a diagnosis of incident cancer (new occurrence of a cancer diagnosis code in proximity to claims for cancer treatment, and no such diagnosis codes during a ≥1 year washout period) during 2014-19, who met additional requirements identifying them as at risk for one of four non-recommended or low value interventions: denosumab for castration sensitive prostate cancer, granulocyte colony stimulating factors (GCSF) for patients at low risk for neutropenic fever, nab-paclitaxel for cancers with no evidence of superiority over paclitaxel, and a branded drug in settings where a generic or biosimilar version was available.
Receipt of the non-recommended or low value drug for which the patient was at risk. The primary association of interest was the assigned oncologist's receipt of any general payments from the manufacturer of the corresponding non-recommended or low value drug (measured in Open Payments) within 365 days before the patient's index cancer date. The two modeling approaches used were general linear model controlling for patients' characteristics and calendar year, and general linear model with physician level indicator variables.
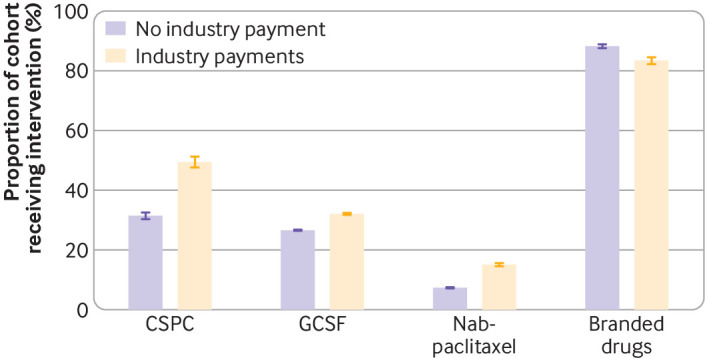
Oncologists were in receipt of industry payments for 2962 of 9799 patients (30.2%) at risk for non-recommended denosumab (median $63), 76 747 of 271 485 patients (28.3%) at risk for GCSF (median $60); 18 491 of 86 394 patients (21.4%) at risk for nab-paclitaxel (median $89), and 4170 of 13 386 patients (31.2%) at risk for branded drugs (median $156). The unadjusted proportion of patients who received non-recommended denosumab was 31.4% for those whose oncologist had not received payment and 49.5% for those whose oncologist had (prevalence difference 18.0%); the corresponding values for GCSF were 26.6% 32.1% (5.5%), for nab-paclitaxel were 7.3% 15.1% (7.8%), and for branded drugs were 88.3% 83.5% (-4.8%). Controlling for patients' characteristics and calendar year, payments from industry were associated with increased use of denosumab (17.5% (95% confidence interval 15.3% to 19.7%)), GCSF (5.8% (5.4% to 6.1%)), and nab-paclitaxel (7.6% (7.1% to 8.1%)), but lower use of branded drugs (-4.6% (-5.8% to -3.3%)). In physician level indicator models, payments from industry were associated with increased use of denosumab (7.4% (2.5% to 12.2%)) and nab-paclitaxel (1.7% (0.9% to 2.5%)), but not with GCSF (0.4% (-0.3% to 1.1%)) or branded drugs (1.2% (-6.0 to 8.5%)).
Within some clinical scenarios, industry payments to physicians are associated with non-recommended and low value drugs. These findings raise quality of care concerns about the financial relationships between physicians and industry.
评估肿瘤医生从制药业获得报酬与患者接受不推荐或低价值干预措施之间的关联。
队列研究。
按服务收费的医疗保险索赔。
2014-19 年期间患有癌症(新发生癌症诊断代码,紧邻癌症治疗索赔,且在≥1 年洗脱期内无此类诊断代码)的医疗保险受益人的诊断数据,他们符合识别出四种不推荐或低价值干预措施之一风险的额外要求:地舒单抗用于去势敏感前列腺癌,粒细胞集落刺激因子(GCSF)用于低风险中性粒细胞减少性发热的患者,白蛋白紫杉醇用于无证据优于紫杉醇的癌症,以及在有通用或生物类似物版本的情况下使用品牌药物。
患者面临风险的不推荐或低价值药物的使用情况。主要关联是指定肿瘤医生在患者指数癌症日期前 365 天内从相应不推荐或低价值药物的制造商处获得任何一般支付(在 Open Payments 中衡量)。使用了两种建模方法,一种是控制患者特征和日历年份的广义线性模型,另一种是包含医生水平指示变量的广义线性模型。
在有风险使用非推荐地舒单抗的 9799 名患者(30.2%)中,肿瘤医生收到了行业支付的 2962 名(中位数 63 美元);在有风险使用 GCSF 的 271485 名患者(28.3%)中,有 76747 名(中位数 60 美元);在有风险使用白蛋白紫杉醇的 86394 名患者(21.4%)中,有 18491 名(中位数 89 美元);在有风险使用品牌药物的 13386 名患者(31.2%)中,有 4170 名(中位数 156 美元)。对于那些肿瘤医生未收到付款的患者,接受非推荐地舒单抗的患者比例为 31.4%,而那些肿瘤医生收到付款的患者比例为 49.5%(患病率差异 18.0%);对于 GCSF,相应的值为 26.6% 32.1%(5.5%),对于白蛋白紫杉醇为 7.3% 15.1%(7.8%),对于品牌药物为 88.3% 83.5%(-4.8%)。在控制患者特征和日历年份后,来自行业的支付与地舒单抗(17.5%(95%置信区间 15.3%至 19.7%))、GCSF(5.8%(5.4%至 6.1%))和白蛋白紫杉醇(7.6%(7.1%至 8.1%))的使用增加有关,但与品牌药物的使用减少有关(-4.6%(-5.8%至 -3.3%))。在医生水平指示模型中,来自行业的支付与地舒单抗(7.4%(2.5%至 12.2%))和白蛋白紫杉醇(1.7%(0.9%至 2.5%))的使用增加有关,但与 GCSF(0.4%(-0.3%至 1.1%))或品牌药物(1.2%(-6.0%至 8.5%))无关。
在某些临床情况下,医生从制药业获得的报酬与不推荐和低价值药物有关。这些发现引发了对医生和制药业之间财务关系的医疗保健质量的关注。