UQ Centre for Clinical Research, The University of Queensland, Brisbane, Queensland, Australia.
Infectious Diseases Unit, Redcliffe Hospital, Redcliffe, Queensland, Australia.
Clin Infect Dis. 2024 Feb 17;78(2):283-291. doi: 10.1093/cid/ciad663.
Persistent Staphylococcus aureus bacteremia is associated with metastatic infection and adverse outcomes, whereas gram-negative bacteremia is normally transient and shorter course therapy is increasingly advocated for affected patients. Whether the prolonged detection of pathogen DNA in blood by culture-independent systems could have prognostic value and guide management decisions is unknown.
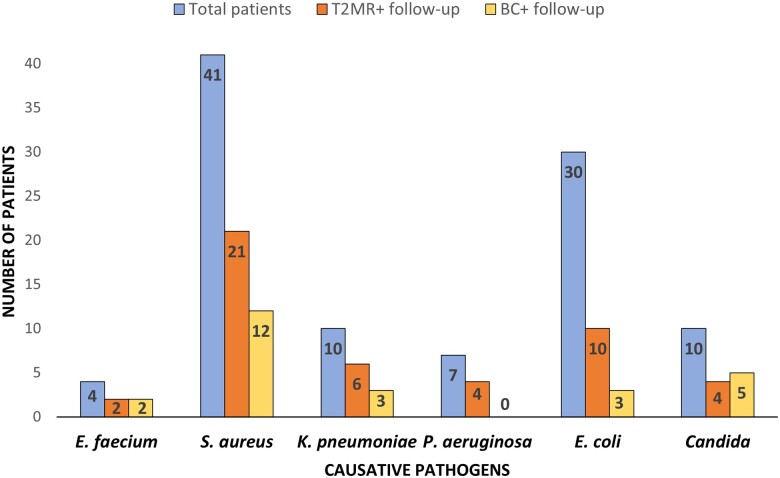
We performed a multicenter, prospective, observational study on 102 patients with bloodstream infection (BSI) to compare time to bloodstream clearance according to T2 magnetic resonance and blood cultures over a 4-day follow-up. We also explored the association between duration of detectable pathogens according to T2 magnetic resonance (magnetic resonance-DNAemia [MR-DNAemia]) and clinical outcomes.
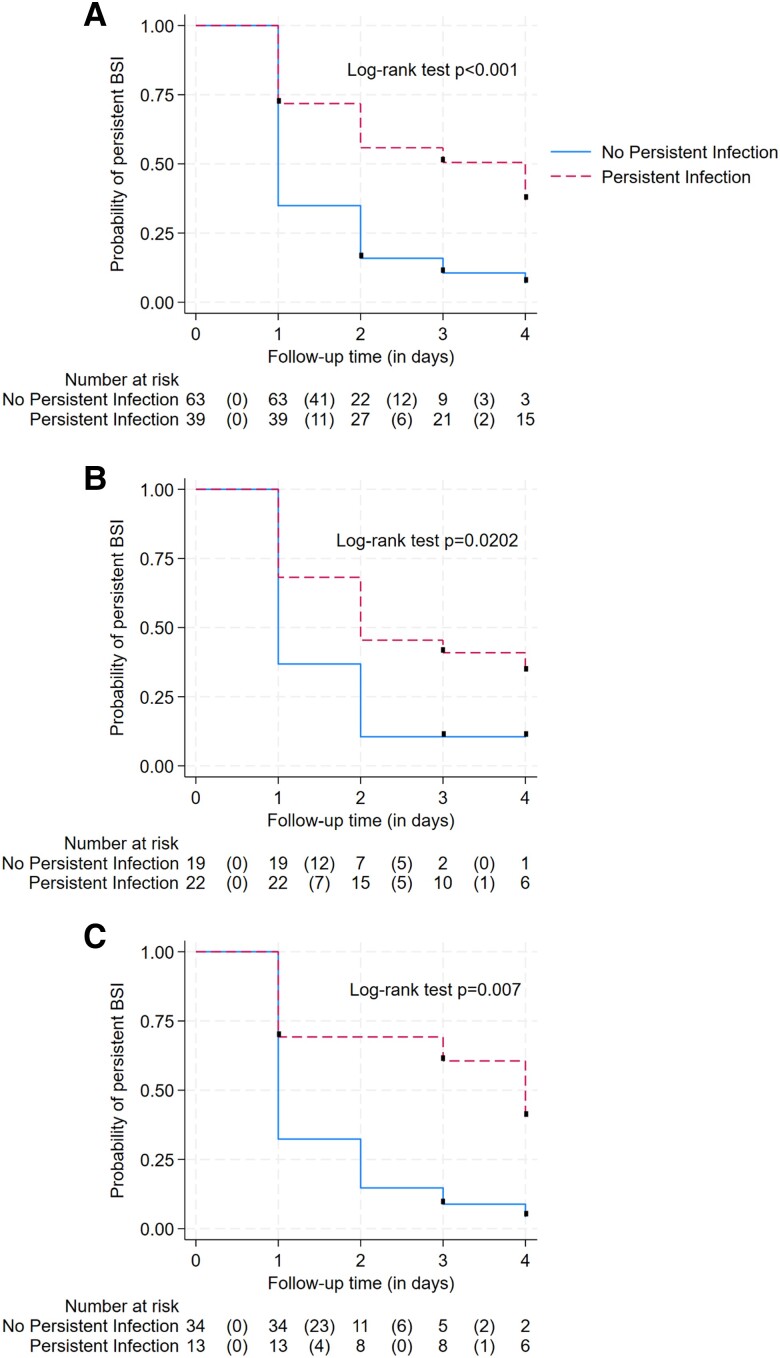
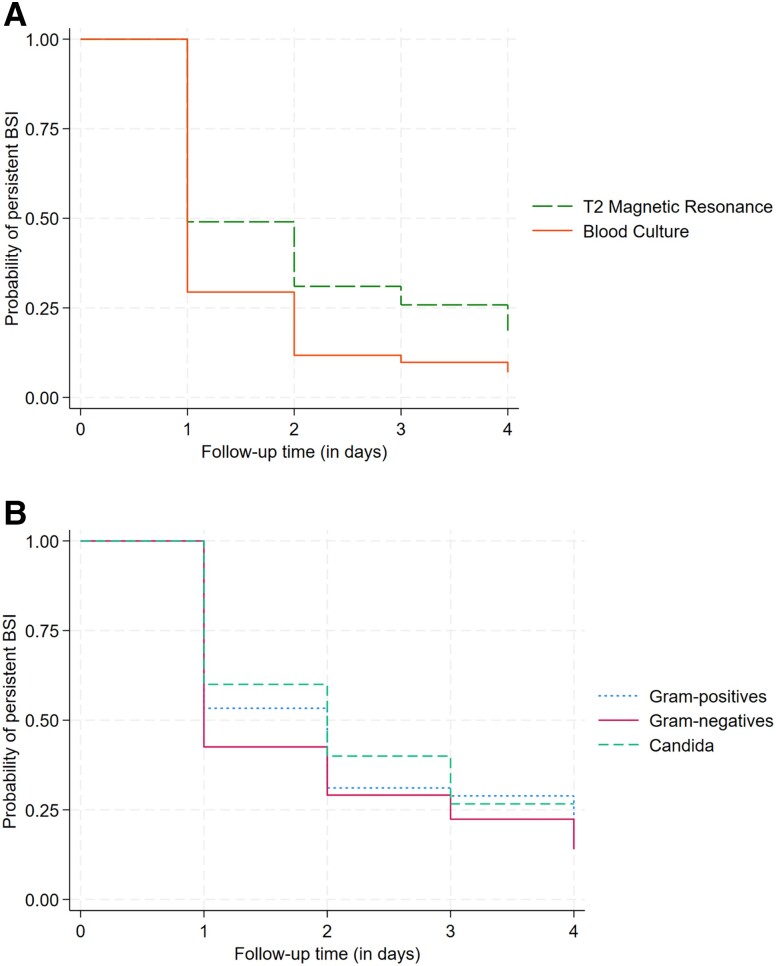
Time to bloodstream clearance according to T2 magnetic resonance was significantly longer than blood culture clearance (HR, .54; 95% CI, .39-.75) and did not differ according to the causative pathogen (P = .5). Each additional day of MR-DNAemia increased the odds of persistent infection (defined as metastatic infection or delayed source control) both in the overall population (OR, 1.98; 95% CI, 1.45-2.70) and in S. aureus (OR, 1.92; 95% CI, 1.12-3.29) and gram-negative bacteremia (OR, 2.21; 95% CI, 1.35-3.60). MR-DNAemia duration was also associated with no improvement in Sequential Organ Failure Assessment score at day 7 from infection onset (OR, 1.76; 95% CI, 1.21-2.56).
T2 magnetic resonance may help diagnose BSI in patients on antimicrobials with negative blood cultures as well as to identify patients with metastatic infection, source control failure, or adverse short-term outcome. Future studies may inform its usefulness within the setting of antimicrobial stewardship programs.
金黄色葡萄球菌菌血症持续存在与转移性感染和不良结局相关,而革兰氏阴性菌血症通常是短暂的,越来越提倡对受影响的患者进行较短疗程的治疗。通过非培养系统检测血液中病原体 DNA 的持续时间是否具有预后价值并指导管理决策尚不清楚。
我们对 102 例血流感染(BSI)患者进行了一项多中心、前瞻性、观察性研究,比较了在 4 天的随访期间,根据 T2 磁共振和血液培养的结果,血液清除的时间。我们还探讨了根据 T2 磁共振(磁共振 DNAemia [MR-DNAemia])检测到的病原体持续时间与临床结局之间的关系。
根据 T2 磁共振的血液清除时间明显长于血培养清除时间(HR,0.54;95%CI,0.39-0.75),且与病原体类型无关(P=0.5)。MR-DNAemia 每增加一天,都会增加持续性感染(定义为转移性感染或延迟源控制)的可能性,无论是在总体人群中(OR,1.98;95%CI,1.45-2.70)还是金黄色葡萄球菌(OR,1.92;95%CI,1.12-3.29)和革兰氏阴性菌血症(OR,2.21;95%CI,1.35-3.60)中。MR-DNAemia 持续时间也与感染发病后第 7 天序贯器官衰竭评估评分无改善相关(OR,1.76;95%CI,1.21-2.56)。
T2 磁共振可帮助诊断接受抗生素治疗但血培养阴性的 BSI 患者,并识别转移性感染、源控制失败或不良短期结局的患者。未来的研究可能会证明其在抗生素管理计划中的有用性。