van Dijken Bart R J, Doff Annerieke R, Enting Roelien H, van Laar Peter Jan, Jeltema Hanne-Rinck, Dierckx Rudi A J O, van der Hoorn Anouk
Department of Radiology, Medical Imaging Center, University Medical Center Groningen, University of Groningen, 9700 RB Groningen, The Netherlands.
Department of Neurology, University Medical Center Groningen, University of Groningen, 9700 RB Groningen, The Netherlands.
Cancers (Basel). 2023 Oct 13;15(20):4973. doi: 10.3390/cancers15204973.
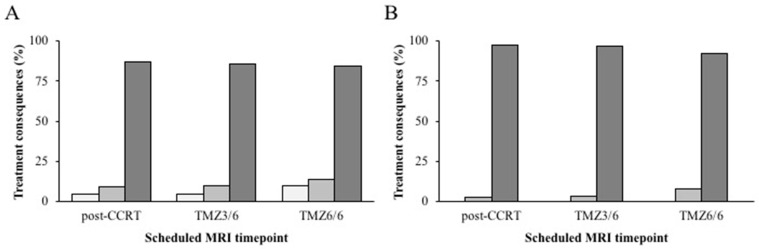
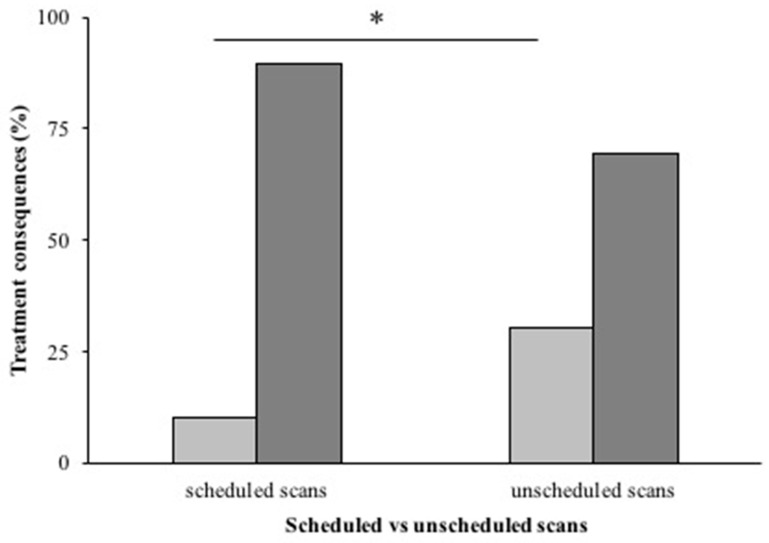
MRI is the gold standard for treatment response assessments for glioblastoma. However, there is no consensus regarding the optimal interval for MRI follow-up during standard treatment. Moreover, a reliable assessment of treatment response is hindered by the occurrence of pseudoprogression. It is unknown if a radiological follow-up strategy at 2-3 month intervals actually benefits patients and how it influences clinical decision making about the continuation or discontinuation of treatment. This study assessed the consequences of scheduled follow-up scans post-chemoradiotherapy (post-CCRT), after three cycles of adjuvant chemotherapy [TMZ3/6], and after the completion of treatment [TMZ6/6]), and of unscheduled scans on treatment decisions during standard concomitant and adjuvant treatment in glioblastoma patients. Additionally, we evaluated how often follow-up scans resulted in diagnostic uncertainty (tumor progression versus pseudoprogression), and whether perfusion MRI improved clinical decision making. Scheduled follow-up scans during standard treatment in glioblastoma patients rarely resulted in an early termination of treatment (2.3% post-CCRT, 3.2% TMZ3/6, and 7.8% TMZ6/6), but introduced diagnostic uncertainty in 27.7% of cases. Unscheduled scans resulted in more major treatment consequences (30%; < 0.001). Perfusion MRI caused less diagnostic uncertainty ( = 0.021) but did not influence treatment consequences ( = 0.871). This study does not support the current pragmatic follow-up strategy and suggests a more tailored follow-up approach.
磁共振成像(MRI)是胶质母细胞瘤治疗反应评估的金标准。然而,对于标准治疗期间MRI随访的最佳间隔尚无共识。此外,假性进展的发生阻碍了对治疗反应的可靠评估。目前尚不清楚每2 - 3个月进行一次放射学随访策略是否真的对患者有益,以及它如何影响关于治疗继续或停止的临床决策。本研究评估了胶质母细胞瘤患者在同步放化疗后(同步放化疗后)、三个周期辅助化疗后(替莫唑胺3/6)以及治疗完成后(替莫唑胺6/6)进行计划内扫描的后果,以及计划外扫描对标准同步和辅助治疗期间治疗决策的影响。此外,我们评估了随访扫描导致诊断不确定性(肿瘤进展与假性进展)的频率,以及灌注MRI是否改善了临床决策。胶质母细胞瘤患者在标准治疗期间进行的计划内随访扫描很少导致治疗提前终止(同步放化疗后为2.3%,替莫唑胺3/6为3.2%,替莫唑胺6/6为7.8%),但在27.7%的病例中引入了诊断不确定性。计划外扫描导致更多重大治疗后果(30%;P < 0.001)。灌注MRI导致的诊断不确定性较小(P = 0.021),但不影响治疗后果(P = 0.871)。本研究不支持当前的实用随访策略,并建议采用更具针对性的随访方法。