Division of Pulmonary and Critical Care Medicine, The Jane and Leonard Korman Respiratory Institute at Thomas Jefferson University, 834 Walnut Street, Suite 650, Philadelphia, PA, 19107, USA.
Department of Medical Oncology, Division of Population Science, Thomas Jefferson University, Philadelphia, PA, 19107, USA.
BMC Health Serv Res. 2023 Oct 30;23(1):1179. doi: 10.1186/s12913-023-10185-4.
Although lung cancer screening (LCS) for high-risk individuals reduces lung cancer mortality in clinical trial settings, many questions remain about how to implement high-quality LCS in real-world programs. With the increasing use of telemedicine in healthcare, studies examining this approach in the context of LCS are urgently needed. We aimed to identify sociodemographic and other factors associated with screening completion among individuals undergoing telemedicine Shared Decision Making (SDM) for LCS.
This retrospective study examined patients who completed Shared Decision Making (SDM) via telemedicine between May 4, 2020 - March 18, 2021 in a centralized LCS program. Individuals were categorized into Complete Screening vs. Incomplete Screening subgroups based on the status of subsequent LDCT completion. A multi-level, multivariate model was constructed to identify factors associated with incomplete screening.
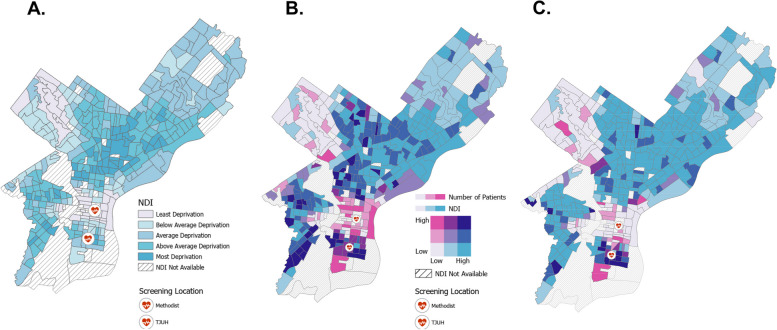
Among individuals undergoing telemedicine SDM during the study period, 20.6% did not complete a LDCT scan. Bivariate analysis demonstrated that Black/African-American race, Medicaid insurance status, and new patient type were associated with greater odds of incomplete screening. On multi-level, multivariate analysis, individuals who were new patients undergoing baseline LDCT or resided in a census tract with a high level of socioeconomic deprivation had significantly higher odds of incomplete screening. Individuals with a greater level of education experienced lower odds of incomplete screening.
Among high-risk individuals undergoing telemedicine SDM for LCS, predictors of incomplete screening included low education, high neighborhood-level deprivation, and new patient type. Future research should focus on testing implementation strategies to improve LDCT completion rates while leveraging telemedicine for high-quality LCS.
虽然在临床试验环境中对高危人群进行肺癌筛查(LCS)可降低肺癌死亡率,但在现实世界的项目中如何实施高质量的 LCS 仍存在许多问题。随着远程医疗在医疗保健中的应用越来越广泛,迫切需要研究这一方法在 LCS 背景下的应用。我们旨在确定与接受远程医疗肺癌筛查共享决策(SDM)的个体的筛查完成相关的社会人口学和其他因素。
本回顾性研究分析了 2020 年 5 月 4 日至 2021 年 3 月 18 日期间在集中式 LCS 计划中通过远程医疗完成 SDM 的患者。根据随后 LDCT 完成情况,将个体分为完全筛查与不完全筛查亚组。构建了一个多层次、多变量模型,以确定与不完全筛查相关的因素。
在研究期间接受远程医疗 SDM 的个体中,有 20.6%未完成 LDCT 扫描。双变量分析表明,黑人/非裔美国人种族、医疗补助保险状况和新患者类型与不完全筛查的可能性更大相关。在多层次、多变量分析中,基线 LDCT 检查或居住在社会经济剥夺程度较高的普查区的新患者,其不完全筛查的可能性显著更高。教育程度较高的个体不完全筛查的可能性较低。
在接受 LCS 远程医疗 SDM 的高危人群中,不完全筛查的预测因素包括教育程度低、邻里剥夺程度高和新患者类型。未来的研究应重点测试实施策略,以提高 LDCT 完成率,同时利用远程医疗实现高质量的 LCS。