Rutgers Cancer Institute, New Brunswick, NJ, USA.
Division of Oncology, Robert Wood Johnson Medical School, Rutgers University, New Brunswick, NJ, USA.
BMC Prim Care. 2024 Oct 18;25(1):373. doi: 10.1186/s12875-024-02610-2.
Lung cancer screening (LCS) can reduce lung cancer mortality but has potential harms for patients. A shared decision-making (SDM) conversation about LCS is required by the Centers for Medicare & Medicaid Services (CMS) for LCS reimbursement. To overcome barriers to SDM in primary care, this protocol describes a telehealth decision coaching and navigation intervention for LCS in primary care clinics delivered by patient navigators. The objective of the study is to evaluate the effectiveness of the intervention and its implementation potential, compared with an enhanced usual care (EUC) arm.
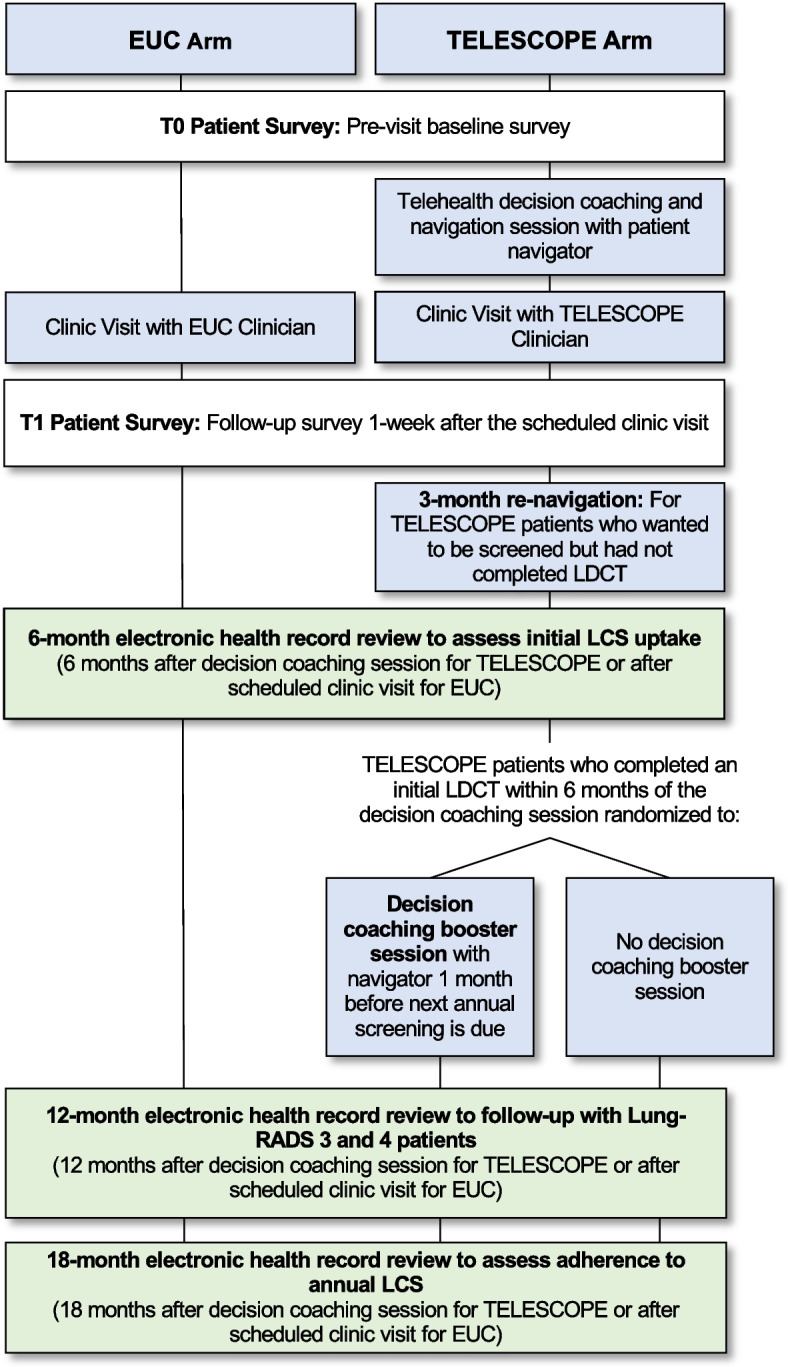
Patients (n = 420) of primary care clinicians (n = 120) are being recruited to a cluster randomized controlled trial. Clinicians are randomly assigned to 1) TELESCOPE intervention: prior to an upcoming non-acute clinic visit, patients participate in a telehealth decision coaching and navigation session about LCS delivered by trained patient navigators and nurse navigators place a low-dose CT scan (LDCT) order for each TELESCOPE patient wanting LCS, or 2) EUC: patients receive enhanced usual care from a clinician. Usual care is enhanced by providing clinicians in both arms with access to a Continuing Medical Education (CME) webinar about LCS and an LCS discussion guide. Patients complete surveys at baseline and 1-week after the scheduled clinic visit to assess quality of the SDM process. Re-navigation is attempted with TELESCOPE patients who have not completed the LDCT within 3 months. One month before being due for an annual screening, TELESCOPE patients whose initial LCS showed low-risk findings are randomly assigned to receive a telehealth decision coaching booster session with a navigator or no booster. Electronic health records are abstracted at 6, 12 and 18 months after the initial decision coaching session (TELESCOPE) or clinic visit (EUC) to assess initial and annual LCS uptake, imaging results, follow-up testing for abnormal findings, cancer diagnoses, treatment, and tobacco treatment referrals. This study will evaluate factors that facilitate or interfere with program implementation using mixed methods.
We will assess whether a decision coaching and patient navigation intervention can feasibly and effectively support high-quality SDM for LCS and guideline-concordant LCS uptake for patients in busy primary care practices serving diverse patient populations.
This study was registered at ClinicalTrials.gov (NCT05491213) on August 4, 2022.
Version 1, April 10, 2024.
肺癌筛查 (LCS) 可以降低肺癌死亡率,但对患者也存在潜在危害。医疗保险和医疗补助服务中心 (CMS) 要求进行 LCS 报销的 SDM 对话。为了克服初级保健中 SDM 的障碍,本方案描述了一种由患者导航员提供的用于初级保健诊所的远程医疗决策辅导和导航干预措施,用于 LCS。该研究的目的是评估干预措施的有效性及其实施潜力,与增强的常规护理 (EUC) 组相比。
正在招募 120 名初级保健临床医生的 420 名患者(n = 420)参加一项集群随机对照试验。临床医生被随机分配到 1)TELESCOPE 干预组:在即将进行的非急性诊所就诊前,患者参加由经过培训的患者导航员和护士导航员进行的关于 LCS 的远程医疗决策辅导和导航会议,每位希望进行 LCS 的 TELESCOPE 患者的导航员都会下达低剂量 CT 扫描 (LDCT) 订单,或 2)EUC:患者接受临床医生的增强常规护理。通过为两个组的临床医生提供关于 LCS 的继续医学教育 (CME) 网络研讨会和 LCS 讨论指南,增强了常规护理。患者在基线和计划就诊后 1 周完成调查,以评估 SDM 过程的质量。对在 3 个月内未完成 LDCT 的 TELESCOPE 患者进行重新导航。在进行年度筛查前 1 个月,初始 LCS 结果显示低风险的 TELESCOPE 患者被随机分配接受与导航员进行的远程医疗决策辅导强化会议或不进行强化辅导。在初始决策辅导会议 (TELESCOPE) 或诊所就诊 (EUC) 后 6、12 和 18 个月,从电子健康记录中提取初始和年度 LCS 参与率、影像学结果、异常发现的随访检查、癌症诊断、治疗和烟草治疗转诊的信息。本研究将使用混合方法评估促进或干扰计划实施的因素。
我们将评估决策辅导和患者导航干预措施是否能够切实有效地支持繁忙的初级保健实践中为患者提供高质量的 LCS 和符合指南的 LCS 参与率,这些实践服务于不同的患者群体。
该研究于 2022 年 8 月 4 日在 ClinicalTrials.gov(NCT05491213)注册。
第 1 版,2024 年 4 月 10 日。