Department of Neurosurgery, Alder Hey Children's Hospital NHS Foundation Trust, Liverpool, UK.
Department of Neurosurgery, The Walton Centre NHS Foundation Trust, Liverpool, UK.
Childs Nerv Syst. 2024 Mar;40(3):665-671. doi: 10.1007/s00381-023-06214-6. Epub 2023 Nov 12.
Neuro-endoscopic lavage (NEL) is an increasingly popular intervention for intraventricular haemorrhage (IVH) and post-haemorrhagic hydrocephalus (PHH), with considerable variation in technique dependent on clinician and clinical circumstances. Whilst efforts to standardise the technique are ongoing, this work describes a tertiary centre experience utilising NEL, highlighting potential caveats to standardisation.
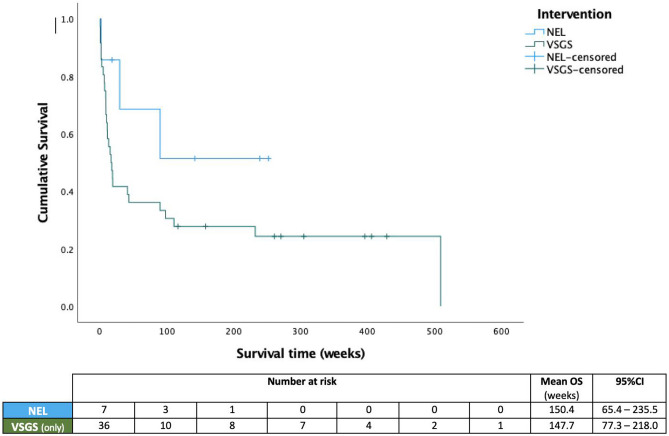
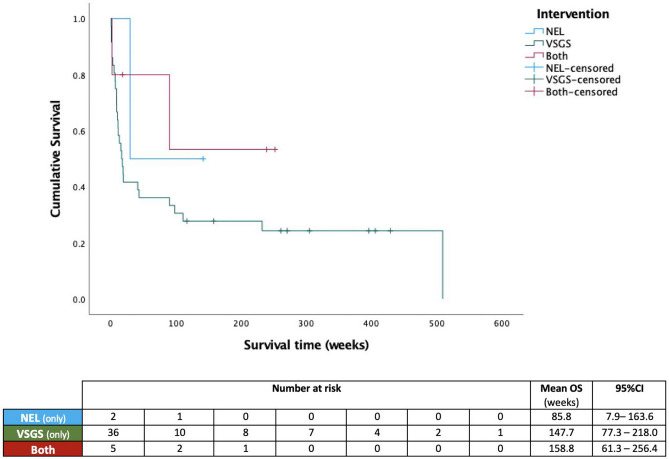
A retrospective review of electronic case notes for patients undergoing temporising surgical intervention for IVH between 2012 and 2021 at our centre was performed. Data collected included (i) gestational age, (ii) aetiology of hydrocephalus, (iii) age at time of intervention, (iv) intervention performed, (v) need for permanent CSF diversion, (vi) 'surgical burden', i.e. number of procedures following primary intervention, and (vii) wound failure and infection rate. Data was handled in Microsoft Excel and statistical analysis SPSS v27.0 RESULTS: 49 neonates (n = 25 males) were included. Overall mean gestational age was 27 weeks and at intervention 35 + 3 weeks. IVH was the predominant cause of hydrocephalus (93.8%) and primary surgical interventions included insertion of a ventriculosubgaleal shunt (VSGS) in n = 41 (83.6%) patients, NEL in n = 6 (12.2%) patients and insertion of an EVD in n = 2 (4.1%). N = 9 (18.4%) patients underwent NEL at some point during the time interval reviewed; n = 4 (8.2%) received NEL monotherapy and n = 5 (10.2%) also received a VSGS. Rate of conversion to definitive CSF diversion between NEL (n = 8, 88.9%) and VSGS cohorts (n = 37, 92.5%) was not significantly different (p = 0.57), nor between NEL alone (n = 3, 75%) and NEL + VSGS (n = 5, 100%) (p = 0.44). None of the patients that underwent NEL monotherapy had any wound issues or CNS infection as a result of the initial intervention, compared to n = 3 (60%) of those that underwent NEL and implantation of VSGS (p = 0.1).
Both NEL and VSGS are effective in temporising hydrocephalus in neonates, occasionally offering a definitive solution in and of themselves. The benefit of dual therapy however remains to be seen, with the addition of VSGS potentially increasing the risk of wound failure in an already vulnerable cohort.
神经内镜灌洗(NEL)是一种越来越受欢迎的治疗脑室出血(IVH)和出血后脑积水(PHH)的方法,其技术因临床医生和临床情况的不同而有很大差异。虽然目前正在努力标准化该技术,但本研究描述了一个利用 NEL 的三级中心经验,强调了标准化的潜在注意事项。
对 2012 年至 2021 年期间在我们中心接受 IVH 临时手术干预的患者的电子病历进行回顾性分析。收集的数据包括(i)胎龄,(ii)脑积水的病因,(iii)干预时的年龄,(iv)干预措施,(v)是否需要永久性脑脊液分流,(vi)“手术负担”,即初级干预后进行的程序数量,以及(vii)伤口失败和感染率。数据在 Microsoft Excel 中处理,并使用 SPSS v27.0 进行统计分析。
共纳入 49 例新生儿(n=25 例男性)。总体平均胎龄为 27 周,干预时为 35+3 周。IVH 是脑积水的主要原因(93.8%),主要的手术干预措施包括脑室-皮下分流管(VSGS)植入术(n=41,83.6%)、NEL(n=6,12.2%)和 EVD 植入术(n=2,4.1%)。n=9(18.4%)患者在研究期间的某个时间点接受了 NEL;n=4(8.2%)患者接受了 NEL 单一疗法,n=5(10.2%)患者接受了 NEL 和 VSGS 联合治疗。NEL 组(n=8,88.9%)和 VSGS 组(n=37,92.5%)之间转换为确定性 CSF 分流的比率无显著差异(p=0.57),NEL 单一疗法组(n=3,75%)和 NEL+VSGS 组(n=5,100%)之间也无显著差异(p=0.44)。与接受 NEL 和 VSGS 联合治疗的患者(n=3,60%)相比,单独接受 NEL 治疗的患者(n=3,75%)均无任何伤口问题或中枢神经系统感染(p=0.1)。
NEL 和 VSGS 均可有效治疗新生儿脑积水,偶尔可作为一种根治方法。然而,双重治疗的益处仍有待观察,联合使用 VSGS 可能会增加在本已脆弱的患者群体中发生伤口失败的风险。