Grande Enrique, Bamias Aristotelis, Galsky Matthew D, Kikuchi Eiji, Davis Ian D, Arranz José Ángel, Rezazadeh Kalebasty Arash, Garcia Del Muro Xavier, Park Se Hoon, De Giorgi Ugo, Alekseev Boris, Mencinger Marina, Izumi Kouji, Puente Javier, Li Jian-Ri, Bernhard Sandrine, Nicholas Alan, Telliez Julie, De Santis Maria
Hospital Ramon y Cajal, Madrid, Spain.
National & Kapodistrian University of Athens, Athens, Greece.
Eur Urol Open Sci. 2023 Nov 4;58:28-36. doi: 10.1016/j.euros.2023.10.002. eCollection 2023 Dec.
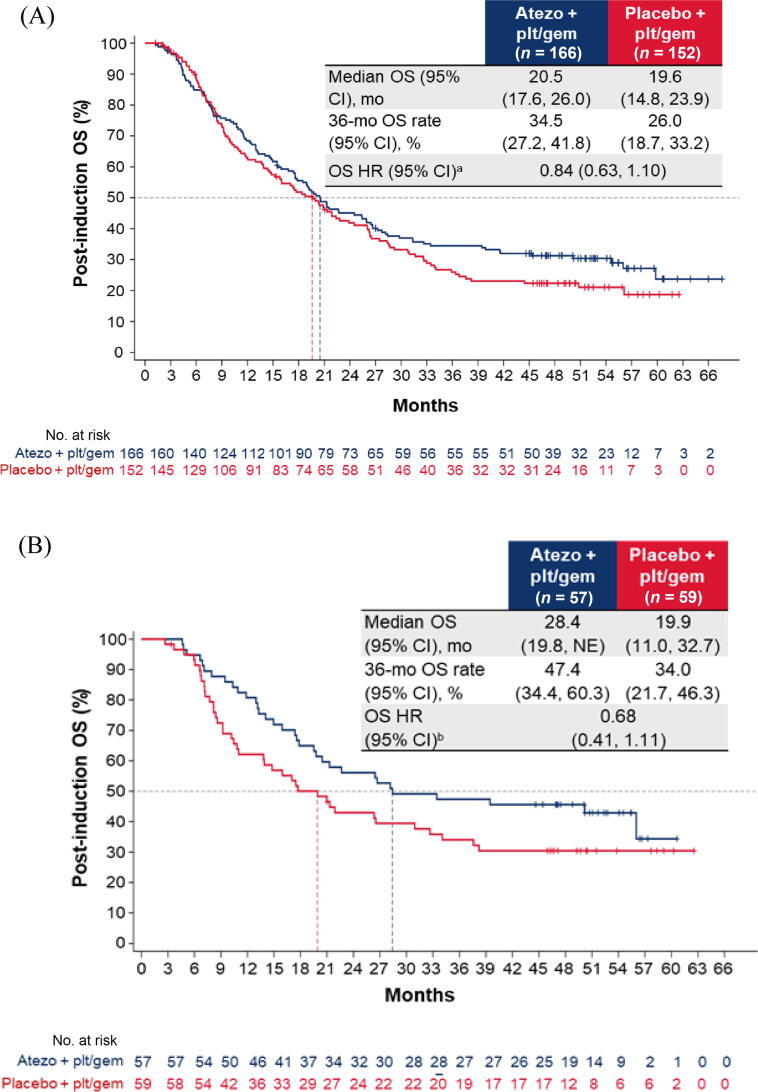
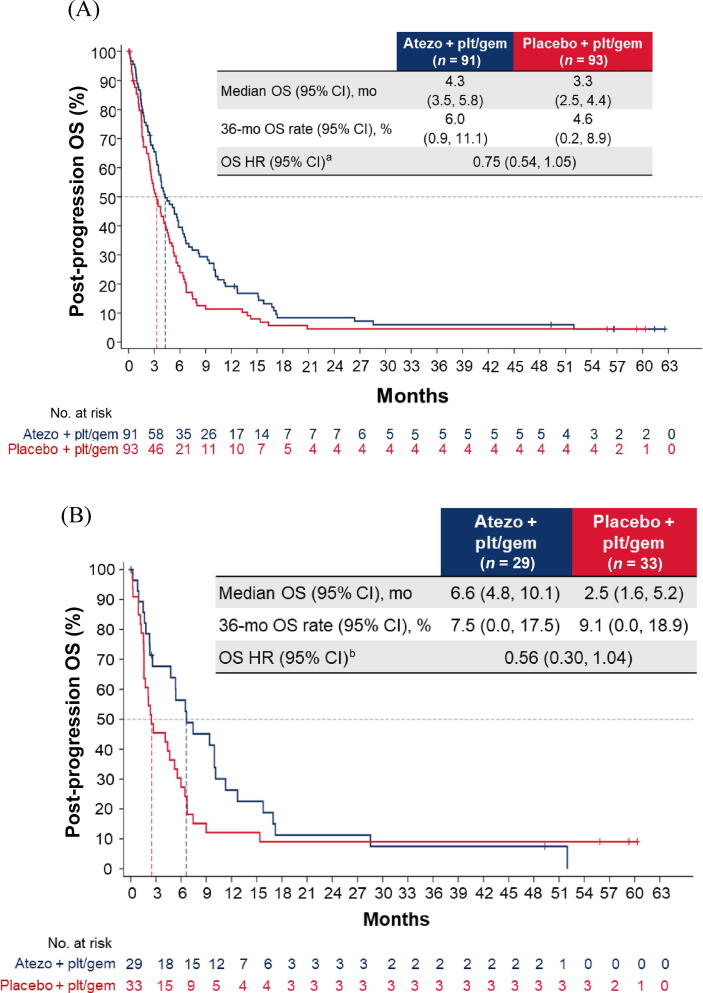
Standard-of-care first-line treatment for metastatic urothelial carcinoma (mUC) is platinum-based chemotherapy (CTx). Maintenance immunotherapy is a treatment option for patients without progressive disease (PD) after induction CTx. IMvigor130 was a randomised, phase 3 study evaluating atezolizumab plus platinum-based CTx (arm A), atezolizumab monotherapy (arm B), or placebo plus platinum-based CTx (arm C) as first-line treatment for mUC. The primary progression-free survival (PFS) analysis showed a statistically significant PFS benefit favouring arm A versus arm C, which did not translate into overall survival (OS) benefit at the final OS analysis. We report exploratory analyses based on response to combination induction treatment (arm A vs arm C) using final OS data. Post-induction OS was analysed for patients without PD during induction (4-6 CTx cycles) who received at least one dose of single-agent atezolizumab/placebo maintenance treatment. Post-progression OS was analysed for patients with PD during induction CTx. Addition of atezolizumab to CTx did not impact OS outcomes, regardless of response to induction CTx, with hazard ratios of 0.84 (95% confidence interval [CI] 0.63-1.10) for patients without PD and 0.75 (95% CI 0.54-1.05) for those with PD during induction CTx. Treatment effects appeared to be greatest for patients treated with cisplatin and for those with PD-L1-high tumours.
The IMvigor130 trial showed that addition of atezolizumab to chemotherapy (CTx) did not improve survival over CTx alone in patients with bladder cancer. Overall, patients whose cancer did not progress during initial treatment tended to live longer than patients whose cancer did progress, but addition of atezolizumab to CTx did not help either group live longer in comparison to CTx alone. However, the results suggest that patients who received a certain CTx drug (cisplatin) or who had high levels of a marker called PD-L1 in their tumour may get the most improvement from addition of atezolizumab to CTx.The IMvigor130 trial is registered on ClinicalTrials.gov as NCT02807636.
转移性尿路上皮癌(mUC)的标准一线治疗是铂类化疗(CTx)。维持性免疫治疗是诱导化疗后无疾病进展(PD)患者的一种治疗选择。IMvigor130是一项随机3期研究,评估阿替利珠单抗联合铂类化疗(A组)、阿替利珠单抗单药治疗(B组)或安慰剂联合铂类化疗(C组)作为mUC的一线治疗。主要无进展生存期(PFS)分析显示,A组与C组相比,PFS有统计学显著获益,但在最终总生存期(OS)分析中未转化为总生存期获益。我们使用最终OS数据报告基于联合诱导治疗反应(A组与C组)的探索性分析。对诱导期(4 - 6个CTx周期)无PD且接受至少一剂单药阿替利珠单抗/安慰剂维持治疗的患者进行诱导后OS分析。对诱导期CTx期间出现PD的患者进行进展后OS分析。无论诱导期CTx反应如何,在CTx中添加阿替利珠单抗均不影响OS结果,诱导期CTx无PD患者的风险比为0.84(95%置信区间[CI]0.63 - 1.10),诱导期CTx有PD患者的风险比为0.75(95%CI0.54 - 1.05)。对于接受顺铂治疗的患者和PD - L1高肿瘤患者,治疗效果似乎最大。
IMvigor130试验表明,在膀胱癌患者中,在化疗(CTx)基础上加用阿替利珠单抗并不能比单纯CTx提高生存率。总体而言,初始治疗期间癌症未进展的患者往往比癌症进展的患者活得更长,但与单纯CTx相比,在CTx中添加阿替利珠单抗对两组患者的生存期延长均无帮助。然而,结果表明,接受某种CTx药物(顺铂)治疗或肿瘤中名为PD - L1的标志物水平高的患者,在CTx中添加阿替利珠单抗可能获益最大。IMvigor130试验在ClinicalTrials.gov上注册为NCT02807636。