School of Public Health, North China University of Science and Technology, Caofeidian Eco-city, Tangshan, Hebei, China.
Department of Cardiology, Kailuan General Hospital, Tangshan, Hebei, China.
JAMA Netw Open. 2023 Nov 1;6(11):e2342831. doi: 10.1001/jamanetworkopen.2023.42831.
Although a high body mass index (BMI) has been found to be associated with increased risk of cardiac conduction block (CCB) in older adults, no further studies have investigated the association between obesity and CCB in the general population.
To investigate the association between obesity and CCB, including its subtypes.
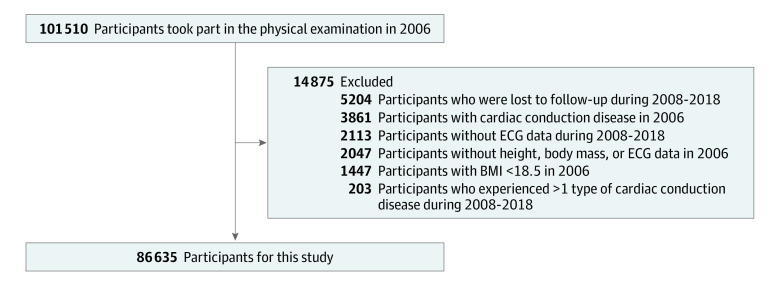
DESIGN, SETTING, AND PARTICIPANTS: This cohort study used data from participants in the Kailuan Study in China (2006-2018) who had completed a physical examination in 2006 (baseline) and had not experienced CCB before baseline. Data analysis was conducted from March to September 2023.
Obesity status was defined by BMI in 3 groups: normal weight (18.5 to <24), overweight (24 to <28), and obesity (≥28).
The primary outcome was CCB, which was diagnosed from standard 12-lead electrocardiography. The primary end point included high-grade atrioventricular block (HAVB), complete right bundle branch block, complete left bundle branch block, left anterior fascicular block (LAFB), and left posterior fascicular block. First-degree atrioventricular block (FAVB), second-degree type 1 AVB, HAVB, complete and incomplete right and left bundle branch block, LAFB, and left posterior fascicular block were considered separately as secondary end points.
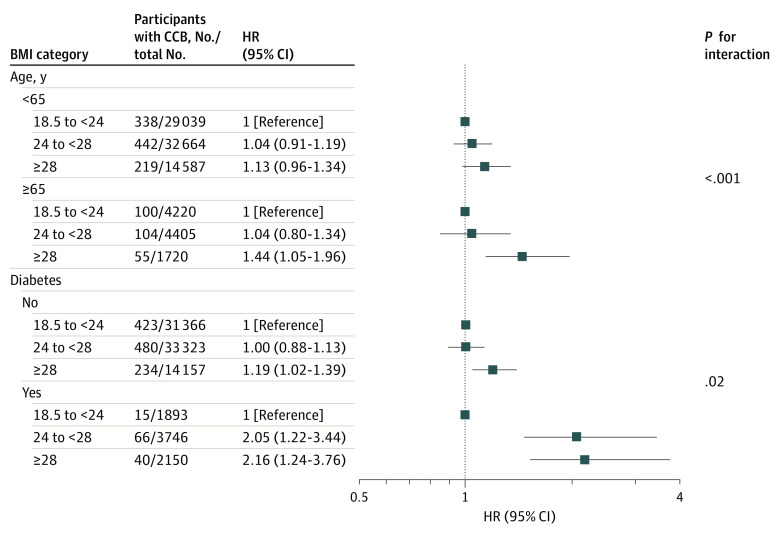
Among 86 635 participants (mean [SD] age, 50.8 [11.9] years; 68 205 males [78.7%]), there were 33 259 individuals with normal weight (38.4%), 37 069 individuals with overweight (42.8%), and 16 307 individuals with obesity (18.8%). The mean (SD) follow-up was 10.6 (3.07) years. In the multivariable Cox proportional hazards regression analysis, obesity was associated with an increased risk of incident CCB (hazard ratio [HR], 1.21; 95% CI, 1.04-1.42) vs normal BMI. In secondary analysis, obesity was associated with an increased risk of FAVB (HR, 1.44; 95% CI, 1.21-1.73), HAVB (HR, 1.99; 95% CI, 1.03-3.82), and LAFB (HR, 1.29; 95% CI, 1.03-1.62) vs normal BMI. There was no association between obesity and other CCB subtypes. Obesity was associated with a greater increase in risk of CCB vs normal BMI in older (aged ≥65 years; HR, 1.44; 95% CI, 1.05-1.96) vs younger (aged <65 years; HR, 1.13; 95% CI, 0.96-1.34) participants (P for interaction < .001) and those with diabetes (HR, 2.16; 95% CI, 1.24-3.76) vs without diabetes (HR, 1.19; 95% CI, 1.02-1.39) (P for interaction = .02).
This study found that obesity was associated with an increased risk of CCB, with greater increases in risk for FAVB, HAVB, and LAFB. Individuals who were older and those who had diabetes had larger increases in risk.
重要性:虽然已有研究发现,较高的体重指数(BMI)与老年人的心脏传导阻滞(CCB)风险增加相关,但尚未有研究进一步调查在普通人群中肥胖与 CCB 之间的关联。
目的:研究肥胖与 CCB 之间的关联,包括其亚型。
设计、地点和参与者:本队列研究使用了来自中国开滦研究的数据(2006-2018 年),这些参与者在 2006 年(基线)完成了体检,且在基线前没有经历过 CCB。数据分析于 2023 年 3 月至 9 月进行。
暴露因素:肥胖状况通过 BMI 分为 3 组:正常体重(18.5 至<24)、超重(24 至<28)和肥胖(≥28)。
主要结果和测量:主要结局为 CCB,通过标准 12 导联心电图诊断。主要终点包括高度房室传导阻滞(HAVB)、完全性右束支传导阻滞、完全性左束支传导阻滞、左前分支阻滞(LAFB)和左后分支阻滞。一度房室传导阻滞(FAVB)、二度 1 型房室传导阻滞、HAVB、完全性和不完全性右束支和左束支传导阻滞、LAFB 和左后分支阻滞分别作为次要终点。
结果:在 86635 名参与者(平均[标准差]年龄,50.8[11.9]岁;68205 名男性[78.7%])中,有 33259 名参与者体重正常(38.4%),37069 名参与者超重(42.8%),16307 名参与者肥胖(18.8%)。平均(标准差)随访时间为 10.6(3.07)年。在多变量 Cox 比例风险回归分析中,与正常 BMI 相比,肥胖与 CCB 事件的发生风险增加相关(风险比[HR],1.21;95%置信区间[CI],1.04-1.42)。在二级分析中,与正常 BMI 相比,肥胖与 FAVB(HR,1.44;95%CI,1.21-1.73)、HAVB(HR,1.99;95%CI,1.03-3.82)和 LAFB(HR,1.29;95%CI,1.03-1.62)的发生风险增加相关。肥胖与其他 CCB 亚型之间无关联。与正常 BMI 相比,肥胖与 CCB 的发生风险增加在年龄较大(≥65 岁;HR,1.44;95%CI,1.05-1.96)与年龄较小(<65 岁;HR,1.13;95%CI,0.96-1.34)的参与者(P 交互<0.001)和患有糖尿病(HR,2.16;95%CI,1.24-3.76)与未患糖尿病(HR,1.19;95%CI,1.02-1.39)的参与者(P 交互=0.02)之间存在差异。
结论和相关性:本研究发现肥胖与 CCB 风险增加相关,与 FAVB、HAVB 和 LAFB 的风险增加更为相关。年龄较大和患有糖尿病的个体风险增加幅度更大。