May Heather P, Herges Joseph R, Anderson Brenda K, Hanson Gregory J, Kashani Kianoush B, Kattah Andrea G, Cole Kristin C, McCoy Rozalina G, Meade Laurie A, Rule Andrew D, Schreier Diana J, Tinaglia Angeliki G, Barreto Erin F
Department of Pharmacy, Mayo Clinic, Rochester, MN.
Anesthesia Clinical Research Unit, Mayo Clinic, Rochester, MN.
Kidney Med. 2023 Oct 5;5(12):100734. doi: 10.1016/j.xkme.2023.100734. eCollection 2023 Dec.
RATIONALE & OBJECTIVE: Innovative models are needed to address significant gaps in kidney care follow-up for acute kidney injury (AKI) survivors.
This quasi-experimental pilot study reports the feasibility of the AKI in Care Transitions (ACT) program, a multidisciplinary approach to AKI survivor care based in the primary care setting.
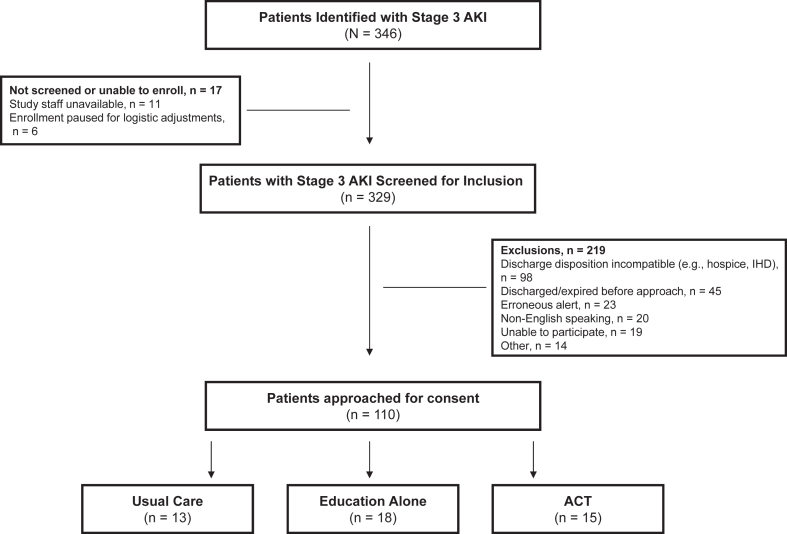
SETTING & PARTICIPANTS: The study included consenting adults with stage 3 AKI discharged home without dialysis.
The ACT intervention included predischarge education from nurses and coordinated postdischarge follow-up with a primary care provider and pharmacist within 14 days. ACT was implemented in phases (Usual Care, Education, ACT).
The primary outcome was feasibility. Secondary outcomes included process and clinical outcomes.
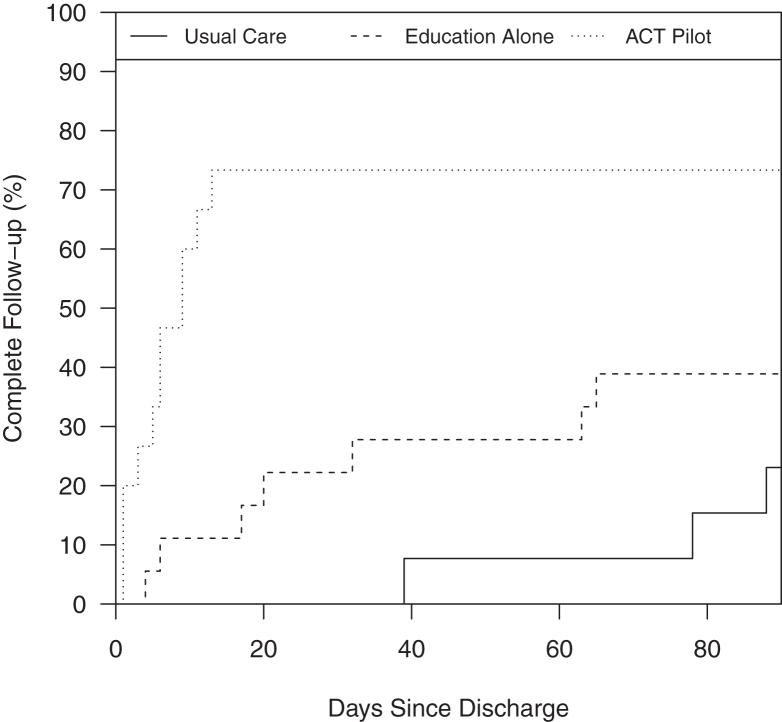
In total, 46 of 110 eligible adults were enrolled. Education occurred in 18/18 and 14/15 participants in the Education and ACT groups, respectively. 30-day urine protein evaluation occurred in 15%, 28%, and 87% of the Usual Care, Education, and ACT groups, respectively ( < 0.001). Cumulative incidence of provider (primary care or nephrologist) and laboratory follow-up at 14 and 30 days was different across groups (14 days: Usual care 0%, Education 11%, ACT 73% [ < 0.01]; 30 days: 0%, 22%, and 73% [ < 0.01]). 30-day readmission rates were 23%, 44%, and 13% in the Usual Care, Education, and ACT groups, respectively ( = 0.13).
Patients were not randomly assigned to treatment groups. The sample size limited the ability to detect some differences or perform multivariable analysis.
This study demonstrated the feasibility of multidisciplinary AKI survivor follow-up beginning in primary care. We observed a higher cumulative incidence of laboratory and provider follow-up in ACT participants.
ClinicalTrials.gov (NCT04505891).
PLAIN-LANGUAGE SUMMARY: Abrupt loss of kidney function in hospitalized patients, acute kidney injury (AKI), increases the chances of long-term kidney disease and a worse health care experience for patients. One out of 3 people who experience AKI do not get the follow-up kidney care they need. We performed a pilot study to test whether a program that facilitates structured AKI follow-up in primary care called the AKI in Care Transitions (ACT) program was possible. ACT brings together the unique expertise of nurses, doctors, and pharmacists to look at the patient's kidney health plan from all angles. The study found that the ACT program was possible and led to more complete kidney care follow-up after discharge than the normal approach to care.
需要创新模式来解决急性肾损伤(AKI)幸存者肾脏护理随访方面的重大差距。
这项准实验性试点研究报告了“急性肾损伤护理过渡(ACT)计划”的可行性,这是一种基于初级保健机构的多学科AKI幸存者护理方法。
该研究纳入了同意参与的3期AKI成年患者,这些患者出院时未进行透析。
ACT干预包括护士在出院前进行教育,并在出院后14天内与初级保健提供者和药剂师进行协调的随访。ACT分阶段实施(常规护理、教育、ACT)。
主要结果是可行性。次要结果包括过程和临床结果。
在110名符合条件的成年人中,共有46人入组。教育分别在教育组的18/18名参与者和ACT组的14/15名参与者中进行。常规护理组、教育组和ACT组分别有15%、28%和87%的患者进行了30天尿蛋白评估(P<0.001)。各治疗组在14天和30天时提供者(初级保健医生或肾病专家)随访和实验室随访的累积发生率不同(14天:常规护理组0%,教育组11%,ACT组73%[P<0.01];30天:0%,22%,73%[P<0.01])。常规护理组、教育组和ACT组的30天再入院率分别为23%、44%和13%(P=0.13)。
患者未随机分配至治疗组。样本量限制了检测某些差异或进行多变量分析的能力。
本研究证明了在初级保健机构开展多学科AKI幸存者随访的可行性。我们观察到ACT参与者的实验室和提供者随访累积发生率更高。
ClinicalTrials.gov(NCT04505891)。
住院患者急性肾功能突然丧失,即急性肾损伤(AKI),会增加长期肾病的几率,并给患者带来更糟糕的医疗体验。每3名经历AKI的患者中就有1人得不到所需的肾脏后续护理。我们进行了一项试点研究,以测试一项名为“急性肾损伤护理过渡(ACT)计划”的项目是否可行,该项目有助于在初级保健机构进行结构化的AKI随访。ACT汇集了护士、医生和药剂师的独特专业知识,从各个角度审视患者的肾脏健康计划。研究发现,ACT计划是可行的,并且与常规护理方法相比,出院后能带来更全面的肾脏护理随访。