Barreto Erin F, May Heather P, Schreier Diana J, Meade Laurie A, Anderson Brenda K, Rensing Megan E, Ruud Kari L, Kattah Andrea G, Rule Andrew D, McCoy Rozalina G, Finnie Dawn M, Herges Joseph R, Kashani Kianoush B
Department of Pharmacy, Mayo Clinic, Rochester, MN, USA.
Anesthesia Clinical Research Unit, Mayo Clinic, Rochester, MN, USA.
Can J Kidney Health Dis. 2022 Mar 6;9:20543581221081258. doi: 10.1177/20543581221081258. eCollection 2022.
Acute kidney injury (AKI) survivors are at heightened risk for poor short- and long-term health outcomes. Even among those who recover after an AKI episode, the risk for chronic kidney disease is 4- to 6-fold higher than in patients without AKI, underscoring the importance of identifying methods to improve AKI survivorship.
The purpose of this report was to describe the development and feasibility of a novel multidisciplinary approach to caring for AKI survivors at care transitions (ACT).
Observational process improvement initiative.
Single academic medical center in the United States.
The studied population was adults with stage 3 AKI not discharging on dialysis who were established with a primary care provider (PCP) at our institution.
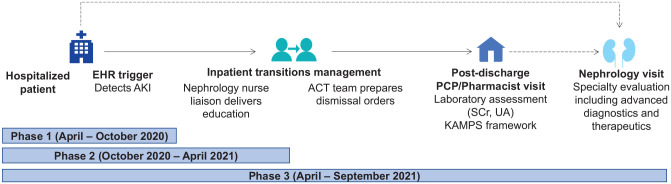
An electronic health record tool was developed prior to implementation to identify AKI survivors. The ACT program encompassed engaging patients in the hospital, delivering education by nephrology-trained nurses before discharge, completing recommended laboratory testing after discharge, and conducting structured kidney-focused follow-up with a pharmacist and a PCP within 7 to 14 days after discharge. Patients could be referred for nephrology evaluation at the discretion of the PCP.
Preliminary data demonstrated that most AKI survivors of interest could be identified, educated, and followed up with this model. This strategy appeared feasible, scalable, and maximized the unique expertise of each member of the multidisciplinary team.
Small sample size, future assessment of process, clinical, and patient-reported outcomes needed.
The multidisciplinary ACT workflow supported by clinical decision support was feasible and addressed gaps in existing care transition models. Team-based care delivery in primary care appears to be a mechanism to extend the capacity for kidney health monitoring for AKI survivors.
急性肾损伤(AKI)幸存者出现短期和长期不良健康结局的风险更高。即使在经历急性肾损伤发作后康复的患者中,患慢性肾病的风险也比未患急性肾损伤的患者高4至6倍,这凸显了确定改善急性肾损伤患者预后方法的重要性。
本报告旨在描述一种新型多学科方法在急性肾损伤幸存者护理过渡(ACT)阶段的开发及可行性。
观察性过程改进计划。
美国一家学术医疗中心。
研究人群为在我院由初级保健医生(PCP)诊治的3期急性肾损伤且未接受透析治疗出院的成年患者。
在实施前开发了一种电子健康记录工具以识别急性肾损伤幸存者。ACT计划包括在医院让患者参与进来,在出院前由经过肾病学培训的护士进行教育,出院后完成推荐的实验室检查,并在出院后7至14天内由药剂师和初级保健医生进行有组织的肾脏专项随访。初级保健医生可酌情将患者转诊进行肾病学评估。
初步数据表明,采用该模型可以识别、教育并随访大多数感兴趣的急性肾损伤幸存者。该策略似乎可行、可扩展,并最大限度地发挥了多学科团队每个成员的独特专业技能。
样本量小,需要对过程、临床及患者报告的结局进行未来评估。
由临床决策支持系统支持的多学科ACT工作流程是可行的,并弥补了现有护理过渡模型中的不足。初级保健中的团队式护理似乎是一种为急性肾损伤幸存者扩展肾脏健康监测能力的机制。