Gritti Michael N, Farid Pedrom, Manlhiot Cedric, Noone Damien, Sakha Seaher, Ali Sam, Bernknopf Bailey, McCrindle Brian W
Labatt Family Heart Centre, Department of Pediatrics, The Hospital for Sick Children, University of Toronto, Toronto, Ontario, Canada.
Department of Pediatrics, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA.
CJC Pediatr Congenit Heart Dis. 2022 Dec 5;2(1):20-29. doi: 10.1016/j.cjcpc.2022.11.007. eCollection 2023 Feb.
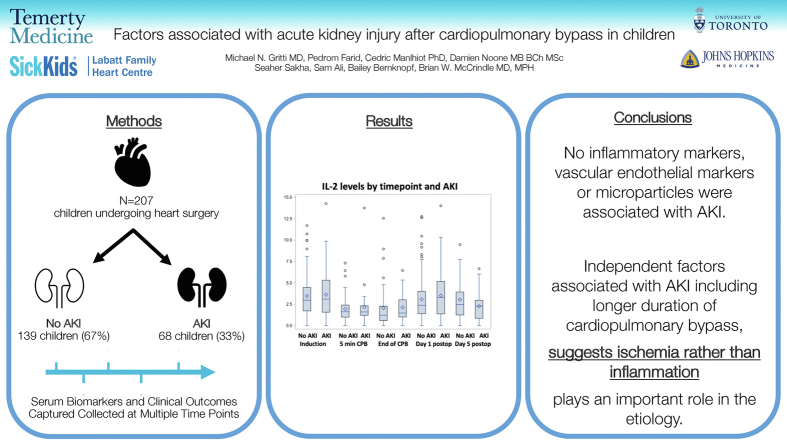
Acute kidney injury (AKI) is a common complication after cardiovascular surgery in children, noted in approximately 40% of children undergoing cardiopulmonary bypass (CPB). We sought to determine the risk factors including inflammatory and vascular endothelial markers associated with AKI in children undergoing cardiac surgery.
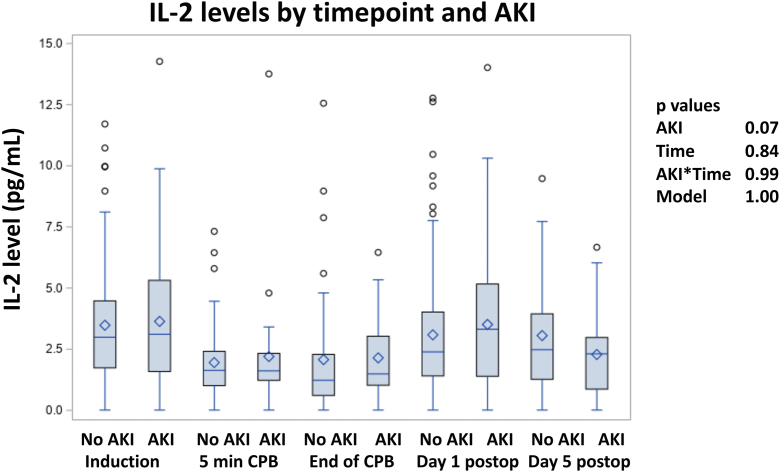
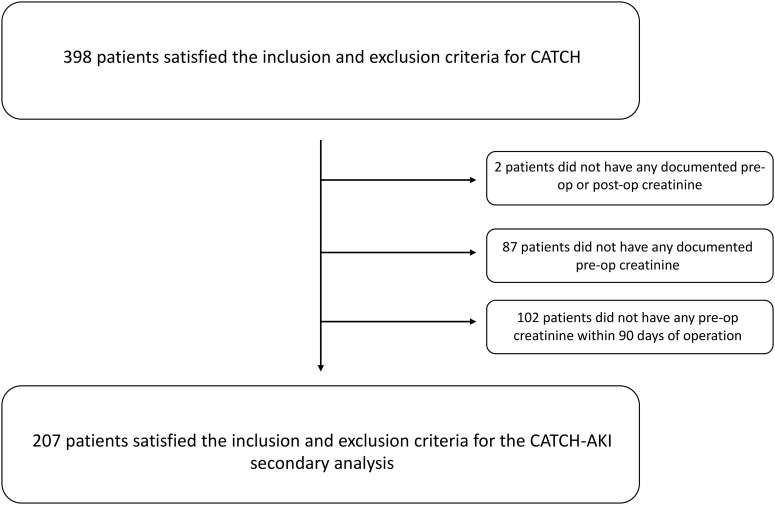
A secondary analysis of a prospective observational cohort study of paediatric patients with a cardiac defect requiring CPB and a weight of >2.5 kg was performed. AKI was defined as a 1.5 times increase from the preoperative value in serum creatinine or an absolute increase by ≥0.3 mg/dL (≥26.5 μmol/L). Plasma inflammatory markers (interleukin [IL]-1a, IL-1b, IL-2, IL-4, IL-6, IL-8, IL-10, IL-12p70, and tumour necrosis factor α) and vascular endothelial markers (vascular endothelial growth factor, von Willebrand factor, regulated on activation, normal T-cell expressed and secreted, granulocyte macrophage colony-stimulating factor, monocyte chemoattractant protein-1, platelet-derived growth factor, and microparticles) were assessed at 5 perioperative time points. Associations with AKI were found using generalized linear regression models adjusted for repeated measures.
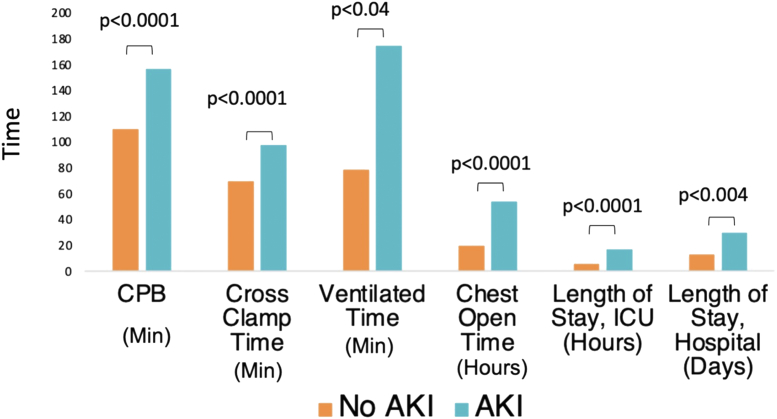
A total of 207 patients were assessed, of whom 56% (n = 116) were male. Thirty-three percent (n = 68) developed AKI. In univariable analyses, adverse outcomes significantly related to the presence of AKI included increased intensive care unit stay (3.0 vs 5.6 hours, < 0.001). In multivariable analysis, independent factors that were significantly associated with AKI included longer duration of CPB (111 vs 154 minutes, < 0.001) and lower preoperative creatinine. Inflammatory and vascular endothelial biomarkers were not associated with AKI.
AKI remains a prevalent problem after cardiac surgery, and renal ischemia related to longer bypass time potentially plays a key role in the etiology. Inflammatory and vascular endothelial biomarkers were not significantly related to AKI.
急性肾损伤(AKI)是儿童心血管手术后常见的并发症,在接受体外循环(CPB)的儿童中约40%会出现。我们试图确定与接受心脏手术的儿童AKI相关的危险因素,包括炎症和血管内皮标志物。
对一项前瞻性观察队列研究进行二次分析,该研究对象为体重>2.5 kg且因心脏缺陷需要CPB的儿科患者。AKI定义为血清肌酐较术前值升高1.5倍或绝对升高≥0.3 mg/dL(≥26.5 μmol/L)。在围手术期的5个时间点评估血浆炎症标志物(白细胞介素[IL]-1α、IL-1β、IL-2、IL-4、IL-6、IL-8、IL-10、IL-12p70和肿瘤坏死因子α)和血管内皮标志物(血管内皮生长因子、血管性血友病因子、激活后上调、正常T细胞表达和分泌、粒细胞巨噬细胞集落刺激因子、单核细胞趋化蛋白-1、血小板衍生生长因子和微粒)。使用针对重复测量进行调整的广义线性回归模型来发现与AKI的关联。
共评估了207例患者,其中56%(n = 116)为男性。33%(n = 68)发生了AKI。在单变量分析中,与AKI存在显著相关的不良结局包括重症监护病房住院时间延长(3.0对5.6小时,<0.001)。在多变量分析中,与AKI显著相关的独立因素包括CPB时间延长(111对154分钟,<0.001)和术前肌酐水平较低。炎症和血管内皮生物标志物与AKI无关。
AKI仍是心脏手术后的一个普遍问题,与较长体外循环时间相关的肾缺血可能在病因中起关键作用。炎症和血管内皮生物标志物与AKI无显著相关性。