Addad Vanessa Vilani, Palma Lilian Monteiro Pereira, Vaisbich Maria Helena, Pacheco Barbosa Abner Mácola, da Rocha Naila Camila, de Almeida Cardoso Marilia Mastrocolla, de Almeida Juliana Tereza Coneglian, de Paula de Sordi Monica Ap, Machado-Rugolo Juliana, Arantes Lucas Frederico, de Andrade Luis Gustavo Modelli
Department of Internal Medicine - UNESP, Univ Estadual Paulista, Rubião Jr, s/n, Botucatu/SP, 18618-687, Brazil.
Department of Pediatrics, Universidade Estadual de Campinas, R. Tessália Vieira de Camargo, 126 - Cidade Universitária, Campinas/SP, 13083-887, Brazil.
Thromb J. 2023 Nov 22;21(1):119. doi: 10.1186/s12959-023-00564-6.
Thrombotic Microangiopathy (TMA) is a syndrome characterized by the presence of anemia, thrombocytopenia and organ damage and has multiple etiologies. The primary aim is to develop an algorithm to classify TMA (TMA-INSIGHT score).
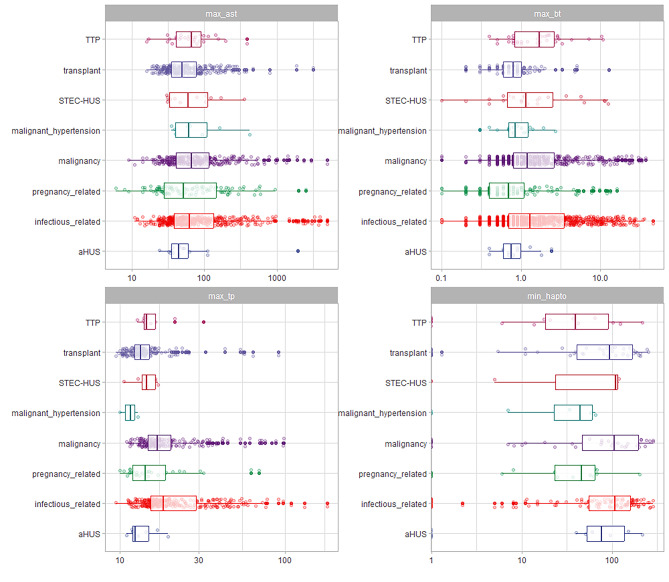
This was a single-center retrospective cohort study including hospitalized patients with TMA at a single center. We included all consecutive patients diagnosed with TMA between 2012 and 2021. TMA was defined based on the presence of anemia (hemoglobin level < 10 g/dL) and thrombocytopenia (platelet count < 150,000/µL), signs of hemolysis, and organ damage. We classified patients in eight categories: infections; Malignant Hypertension; Transplant; Malignancy; Pregnancy; Thrombotic Thrombocytopenic Purpura (TTP); Shiga toxin-mediated hemolytic uremic syndrome (STEC-SHU) and Complement Mediated TMA (aHUS). We fitted a model to classify patients using clinical characteristics, biochemical exams, and mean arterial pressure at presentation.
We retrospectively retrieved TMA phenotypes using automatic strategies in electronic health records in almost 10 years (n = 2407). Secondary TMA was found in 97.5% of the patients. Primary TMA was found in 2.47% of the patients (TTP and aHUS). The best model was LightGBM with accuracy of 0.979, and multiclass ROC-AUC of 0.966. The predictions had higher accuracy in most TMA classes, although the confidence was lower in aHUS and STEC-HUS cases.
Secondary conditions were the most common etiologies of TMA. We retrieved comorbidities, associated conditions, and mean arterial pressure to fit a model to predict TMA and define TMA phenotypic characteristics. This is the first multiclass model to predict TMA including primary and secondary conditions.
血栓性微血管病(TMA)是一种以贫血、血小板减少和器官损害为特征的综合征,病因多样。主要目的是开发一种对TMA进行分类的算法(TMA-INSIGHT评分)。
这是一项单中心回顾性队列研究,纳入了在单一中心住院的TMA患者。我们纳入了2012年至2021年间所有连续诊断为TMA的患者。TMA的定义基于贫血(血红蛋白水平<10 g/dL)、血小板减少(血小板计数<150,000/µL)、溶血迹象和器官损害。我们将患者分为八类:感染;恶性高血压;移植;恶性肿瘤;妊娠;血栓性血小板减少性紫癜(TTP);志贺毒素介导的溶血尿毒综合征(STEC-SHU)和补体介导的TMA(aHUS)。我们使用临床特征、生化检查和就诊时的平均动脉压拟合了一个对患者进行分类的模型。
我们在近10年的电子健康记录中使用自动策略回顾性检索了TMA表型(n = 2407)。97.5%的患者为继发性TMA。2.47%的患者为原发性TMA(TTP和aHUS)。最佳模型是LightGBM,准确率为0.979,多类ROC-AUC为0.966。尽管在aHUS和STEC-HUS病例中预测的置信度较低,但在大多数TMA类别中预测具有更高的准确性。
继发性疾病是TMA最常见的病因。我们检索了合并症、相关疾病和平均动脉压以拟合一个预测TMA并定义TMA表型特征的模型。这是第一个预测包括原发性和继发性疾病的TMA的多类模型。