Schönermarck Ulf, Ries Wolfgang, Schröppel Bernd, Pape Lars, Dunaj-Kazmierowska Malgorzata, Burst Volker, Mitzner Steffen, Basara Nadezda, Starck Michael, Schmidbauer Daniel, Mellmann Alexander, Dittmer Rita, Jeglitsch Michael, Haas Christian S
Medizinische Klinik IV, Klinikum der Universität, LMU, Munich, Germany.
Internal Medicine, Diakonissenkrankenhaus, Flensburg, Germany.
Clin Kidney J. 2019 Jun 18;13(2):208-216. doi: 10.1093/ckj/sfz066. eCollection 2020 Apr.
Data are lacking on the relative incidence of thrombotic thrombocytopenic purpura (TTP), haemolytic uraemic syndrome (HUS) caused by Shiga toxin-producing (STEC) and atypical HUS (aHUS) in patients presenting with thrombotic microangiopathies (TMAs).
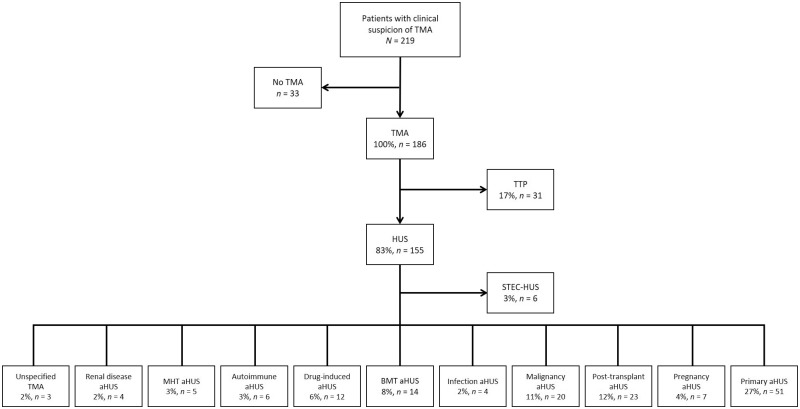
This was a prospective, cross-sectional, multicentre and non-interventional epidemiological study. Patients fulfilling criteria for TMAs (platelet consumption, microangiopathic haemolytic anaemia and organ dysfunction) were included in the study. The primary objective was to assess the relative incidence of TTP, STEC-HUS, aHUS and 'other' physician-defined diagnoses. The secondary objective was to develop an algorithm to predict a severe deficiency in ADAMTS13 (a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13) activity (≤10%) using routine laboratory parameters. A classification using the recent Kidney Disease: Improving Global Outcomes diagnostic criteria was then undertaken to further classify patient groups.
aHUS was diagnosed with a relative incidence of 61%, whereas TTP, STEC-HUS and 'other' were diagnosed in 13, 6 and 20% of patients, respectively. In the analysis, 27% of patients with a TMA were classified as 'primary aHUS' and 53% as 'secondary aHUS'. Multivariate analysis revealed that severe deficiency in ADAMTS13 activity (≤10%) was unlikely to underlie TMA if platelet and serum creatinine were above threshold values of 30 × 10/L and 1.8 mg/dL, respectively (negative predictive value of 92.3 and 98.1, respectively, if one or both values were above the threshold).
In this study, aHUS was the most common single diagnosis among patients presenting with a TMA. In the absence of an ADAMTS13 activity result, platelet count and serum creatinine may aid in the differential diagnosis.
关于血栓性血小板减少性紫癜(TTP)、产志贺毒素大肠杆菌(STEC)所致溶血性尿毒症综合征(HUS)及非典型HUS(aHUS)在血栓性微血管病(TMA)患者中的相对发病率,目前尚无相关数据。
这是一项前瞻性、横断面、多中心的非干预性流行病学研究。符合TMA标准(血小板消耗、微血管病性溶血性贫血及器官功能障碍)的患者纳入本研究。主要目的是评估TTP、STEC-HUS、aHUS及其他医生定义诊断的相对发病率。次要目的是利用常规实验室参数制定一种算法,以预测金属蛋白酶解聚素与血小板反应蛋白1型基序13(ADAMTS13)活性严重缺乏(≤10%)的情况。随后采用最近的《改善全球肾脏病预后组织》诊断标准进行分类,以进一步对患者群体进行分类。
诊断为aHUS的相对发病率为61%,而诊断为TTP、STEC-HUS及其他的患者分别占13%、6%和20%。在分析中,27%的TMA患者被分类为“原发性aHUS”,53%为“继发性aHUS”。多变量分析显示,如果血小板和血清肌酐分别高于30×10⁹/L和1.8mg/dL的阈值,则ADAMTS13活性严重缺乏(≤10%)不太可能是TMA的病因(如果一个或两个值高于阈值,阴性预测值分别为92.3和98.1)。
在本研究中,aHUS是TMA患者中最常见的单一诊断。在缺乏ADAMTS13活性结果的情况下,血小板计数和血清肌酐可能有助于鉴别诊断。