Centre for Inherited Cardiovascular Diseases, Zayed Centre for Research, Great Ormond Street Hospital, Great Ormond Street, London, WC1N 4JH, UK.
Institute of Cardiovascular Sciences, University College London, 62 Huntley St, London, WC1E 6DD, UK.
Europace. 2023 Nov 2;25(11). doi: 10.1093/europace/euad330.
The validated HCM Risk-Kids model provides accurate individualized estimates of sudden cardiac death risk in children with hypertrophic cardiomyopathy (HCM). A second validated model, PRIMaCY, also provides individualized estimates of risk, but its performance and clinical impact has not been independently investigated. The aim of this study was to investigate the clinical impact of using the PRIMaCY sudden cardiac death (SCD) risk model in childhood HCM.
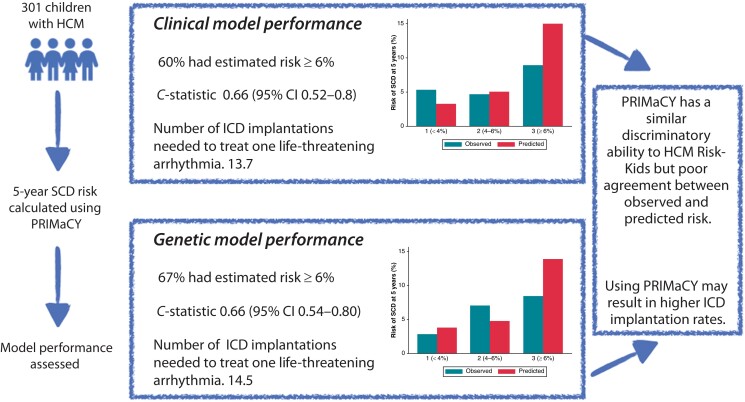
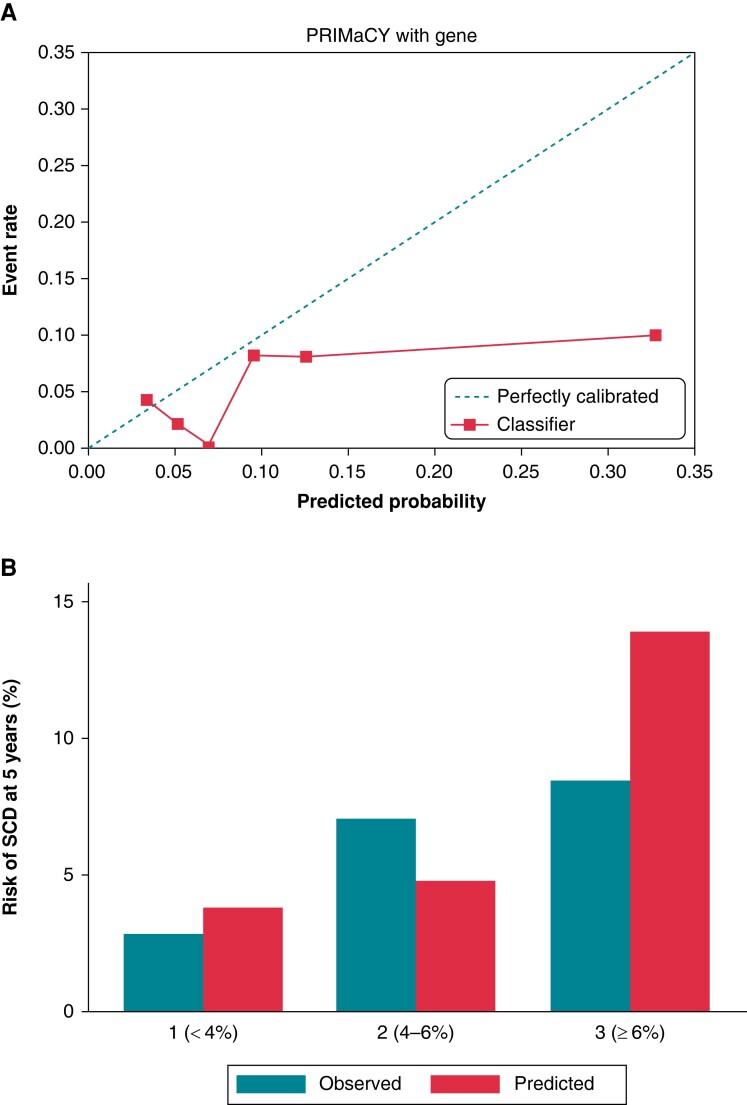
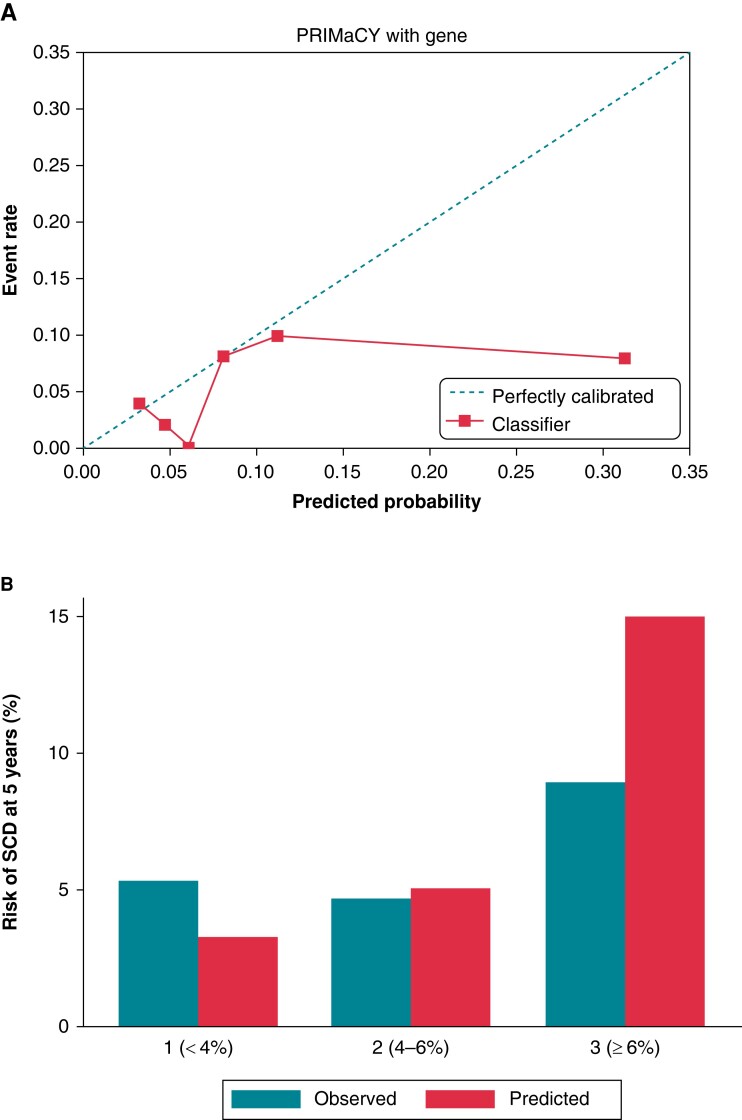
The estimated 5-year SCD risk was calculated for children meeting diagnostic criteria for HCM in a large single-centre cohort using PRIMaCY (clinical and genetic) and HCM Risk-Kids model, and model performance was assessed. Three hundred one patients [median age 10 (interquartile range 4-14)] were followed up for an average of 4.9 (±3.8) years, during which 30 (10.0%) reached the SCD or equivalent event endpoint. Harrell's C-statistic for the clinical and genetic models was 0.66 [95% confidence interval (CI) 0.52-0.8] and 0.66 (95% CI 0.54-0.80) with a calibration slope of 0.19 (95% CI 0.04-0.54) and 0.26 (95% CI -0.03-0.62), respectively. The number needed to treat to potentially treat one life-threatening arrhythmia for the PRIMaCY clinical, PRIMaCY genetic, and HCM Risk-Kids models was 13.7, 14.5, and 9.4, respectively.
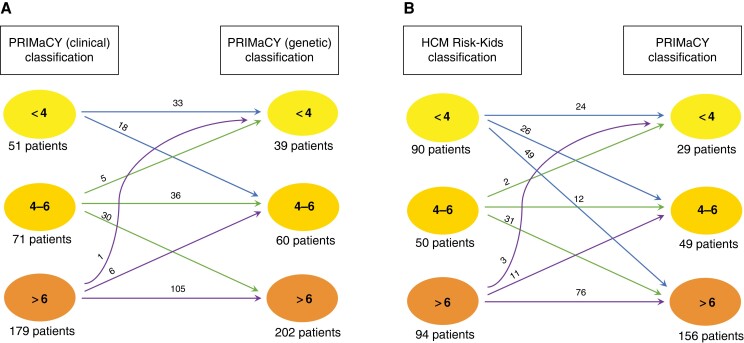
Although PRIMaCY has a similar discriminatory ability to that reported for HCM Risk-Kids, estimated risk estimates did not correlate well with observed risk. A higher proportion of patients met implantable cardioverter-defibrillator thresholds using PRIMaCY model compared with HCM Risk-Kids. This has important clinical implications as these patients will be exposed to a lifetime risk of complications and inappropriate therapies.
经过验证的 HCM Risk-Kids 模型可准确预测肥厚型心肌病(HCM)儿童的心脏性猝死(SCD)风险。另一个经过验证的 PRIMaCY 模型也可以提供个体化的风险估计,但尚未对其性能和临床影响进行独立研究。本研究旨在调查在儿童 HCM 中使用 PRIMaCY SCD 风险模型的临床影响。
使用 PRIMaCY(临床和遗传)和 HCM Risk-Kids 模型计算符合 HCM 诊断标准的大型单中心队列中儿童的 5 年 SCD 风险,并评估模型性能。301 例患者[中位年龄 10 岁(四分位间距 4-14 岁)]平均随访 4.9(±3.8)年,期间 30 例(10.0%)达到 SCD 或等效终点。临床和遗传模型的 Harrell C 统计量分别为 0.66(95%置信区间 0.52-0.8)和 0.66(95%置信区间 0.54-0.80),校准斜率分别为 0.19(95%置信区间 0.04-0.54)和 0.26(95%置信区间 -0.03-0.62)。PRIMaCY 临床、PRIMaCY 遗传和 HCM Risk-Kids 模型的潜在治疗 1 次危及生命的心律失常的治疗人数分别为 13.7、14.5 和 9.4。
尽管 PRIMaCY 的判别能力与 HCM Risk-Kids 相似,但风险估计值与观察到的风险相关性不佳。与 HCM Risk-Kids 相比,更多的患者符合植入式心律转复除颤器的阈值。这具有重要的临床意义,因为这些患者将面临终生并发症和不适当治疗的风险。