Department of Radiation Oncology, Radiation Oncology Key Laboratory of Sichuan Province.
Shandong Cancer Hospital Affiliated to Shandong University.
Int J Surg. 2024 Feb 1;110(2):956-964. doi: 10.1097/JS9.0000000000000912.
There is no standard management for small cell esophageal carcinoma (SCEC). The purpose of this multicenter, retrospective study (ChiSCER) was to investigate the treatment, outcomes, and risk factors impacting survival endpoints in patients with limited-stage SCEC (LS-SCEC).
Consecutive patients with LS-SCEC from 14 institutions between 2000 and 2020 in China were enrolled. Survival curves were constructed using the Kaplan-Meier method and compared using a log-rank test. Univariate and multivariate Cox regression models and propensity score matching (PSM) analysis were adopted in the prognostic analysis. Results were reported as hazard ratio (HR), 95% confidence interval (CI), and P value. Statistical significance was set as P value <0.05 in a two-tailed test.
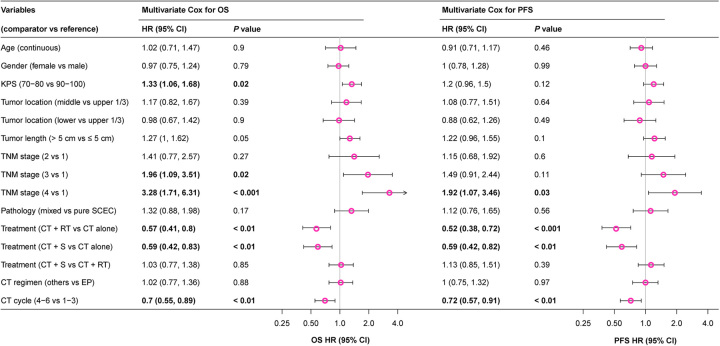
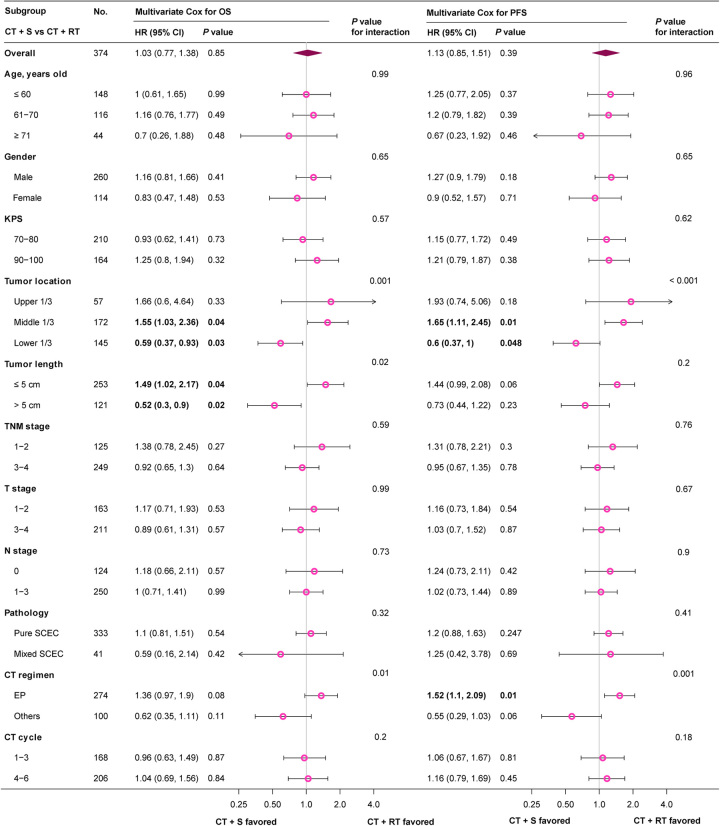
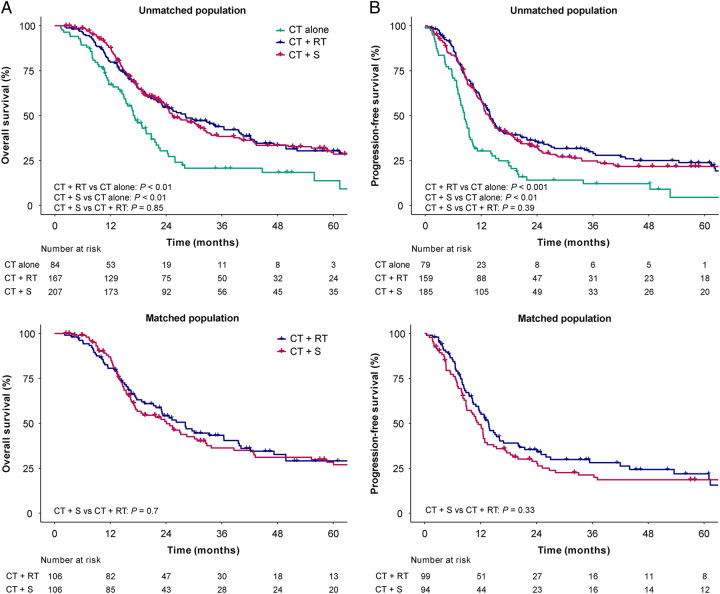
Among 458 LS-SCEC patients, the median age was 63 [interquartile range (IQR), 57-68] years, and 318 (69%) were males. Eighty-four (18%), 167 (36%), and 207 (45%) patients received chemotherapy (CT) alone, CT plus definitive radiotherapy (CT+RT), and CT plus radical surgery (CT+S), respectively. With a median follow-up time of 58.7 (95% CI 48.9-68.6) months, the median overall survival (OS) and 3-year OS rate for all patients 24.3 (95% CI 21.6-27) months and 37.3% (95% CI 32.8-42.5%), respectively. Multivariate analysis indicated that treatment modes, Karnofsky performance status (KPS), TNM stage, and CT cycle were independent prognostic factors for OS ( P <0.05). Compared with CT alone, patients treated with CT+RT (HR 0.57, 95% CI 0.41-0.8, P =0.001) or CT+S (HR 0.59, 95% CI 0.42-0.82, P =0.002) had an improved OS, with no significant survival differences between CT+S and CT+RT groups after multivariate and PSM analyses ( P >0.05). Subgroup analysis indicated that compared with CT+RT, patients with tumor location at lower 1/3 (HR 0.59, 95% CI 0.37-0.93, P =0.03) or tumor length >5 cm (HR 0.52, 95% CI 0.3-0.9, P =0.02) could obtain significant OS benefit from CT+S. Patients with tumor location at middle 1/3 (HR 1.55, 95% CI 1.03-2.36, P =0.04) or tumor length ≤5 cm (HR 1.49, 95% CI 1.02-2.17, P =0.04) favored CT+RT. Distant metastasis accounted for 73.7% of all treatment failures after multidisciplinary treatments.
Surgery and RT were equally effective local therapies for patients with LS-SCEC. The personalized decision of local therapy should be made after comprehensive considerations on tumor location, length, comorbidities, and organ preservation.
目前小细胞食管癌(SCEC)尚无标准治疗方案。本多中心回顾性研究(ChiSCER)旨在探讨局限期小细胞食管癌(LS-SCEC)患者的治疗方法、结局和影响生存终点的风险因素。
纳入 2000 年至 2020 年期间中国 14 家机构的 LS-SCEC 连续患者。采用 Kaplan-Meier 法绘制生存曲线,对数秩检验比较生存曲线。采用单因素和多因素 Cox 回归模型及倾向性评分匹配(PSM)分析进行预后分析。结果以风险比(HR)、95%置信区间(CI)和 P 值表示。双侧检验 P 值<0.05 为差异有统计学意义。
458 例 LS-SCEC 患者中,中位年龄为 63 岁[四分位间距(IQR):57-68 岁],318 例(69%)为男性。84 例(18%)、167 例(36%)和 207 例(45%)患者分别接受单纯化疗(CT)、CT 联合根治性放疗(CT+RT)和 CT 联合根治性手术(CT+S)治疗。中位随访时间为 58.7(95%CI 48.9-68.6)个月,所有患者的中位总生存期(OS)和 3 年 OS 率分别为 24.3(95%CI 21.6-27)个月和 37.3%(95%CI 32.8-42.5%)。多因素分析表明,治疗方式、卡氏功能状态评分(KPS)、TNM 分期和 CT 周期是 OS 的独立预后因素(P<0.05)。与单纯 CT 相比,接受 CT+RT(HR 0.57,95%CI 0.41-0.8,P=0.001)或 CT+S(HR 0.59,95%CI 0.42-0.82,P=0.002)治疗的患者 OS 得到改善,多因素和 PSM 分析后 CT+S 与 CT+RT 组之间无显著生存差异(P>0.05)。亚组分析表明,与 CT+RT 相比,肿瘤位于食管下段 1/3 (HR 0.59,95%CI 0.37-0.93,P=0.03)或肿瘤长度>5 cm(HR 0.52,95%CI 0.3-0.9,P=0.02)的患者可从 CT+S 中获得显著的 OS 获益。肿瘤位于食管中段 1/3 (HR 1.55,95%CI 1.03-2.36,P=0.04)或肿瘤长度≤5 cm(HR 1.49,95%CI 1.02-2.17,P=0.04)的患者更适合接受 CT+RT。多学科治疗后,所有治疗失败中远处转移占 73.7%。
手术和放疗对 LS-SCEC 患者均为有效的局部治疗方法。局部治疗方案的个体化决策应综合考虑肿瘤位置、长度、合并症和器官保留情况。