Nakfa Hospital, Northern Red Sea Ministry of Health Branch, Nakfa, Eritrea.
National Health Observatory Unit, Ministry of Health, Asmara, Eritrea.
Sci Rep. 2023 Nov 27;13(1):20792. doi: 10.1038/s41598-023-47258-7.
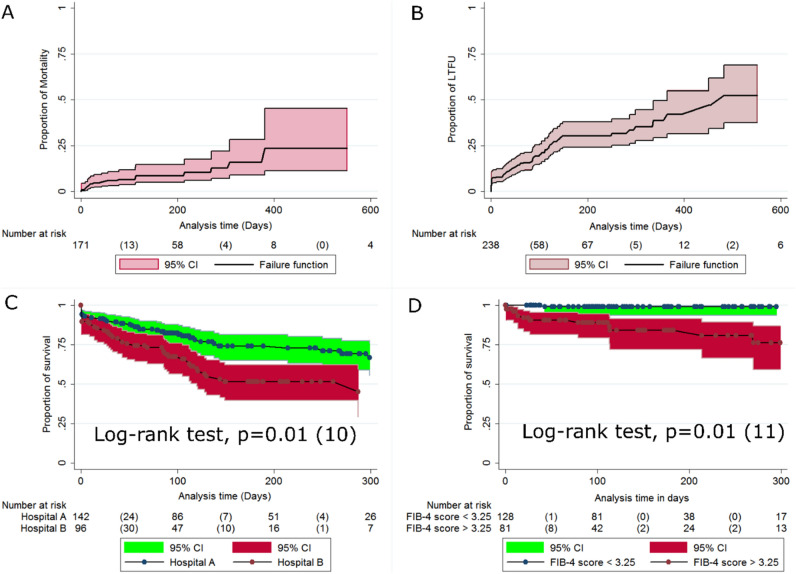
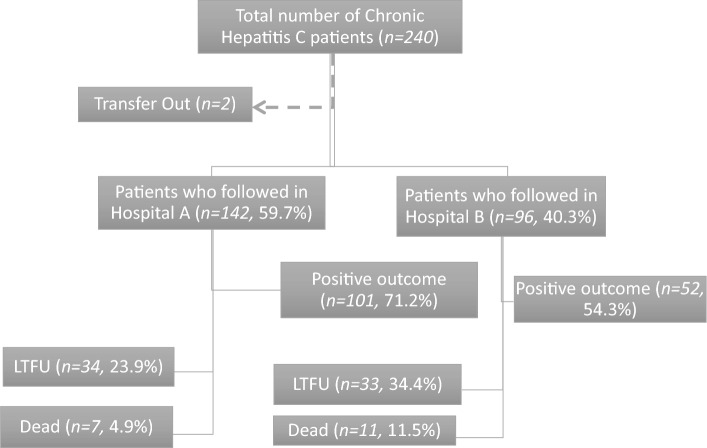
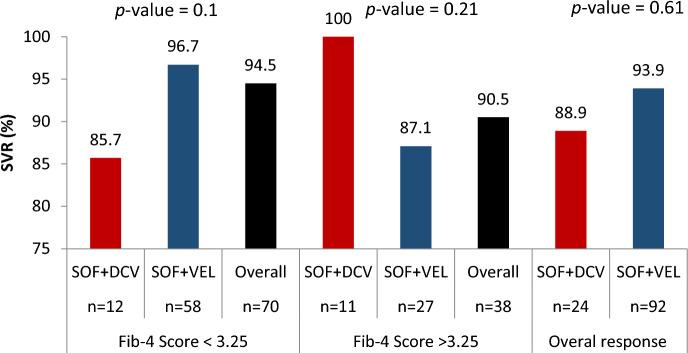
Reliable real-world data on direct acting anti-retroviral (DAA) uptake and treatment outcomes are lacking for patients with hepatitis C virus (HCV) in sub-Saharan Africa. This study provides data on HCV DAA-based treatment outcomes, mortality, loss-to-follow up, and associated factors among patients in Eritrea. A multicenter retrospective observational cohort study was conducted in two tertiary hospitals in Asmara, Eritrea. A structured checklist was used to collect data from patient's cards. Descriptive and inferential statistics used included means (± Standard deviation (SD), medians (Interquartile range (IQR), chi-squire (χ), Kaplan-Meier estimates, and multivariate Cox proportional hazard models. A total of 238 patients with median age of 59 years (IQR 50-69 years) were enrolled in the study. Out of the 227 patients initiated on treatment, 125 patients had viral load measurements at 12 weeks after end of treatment (EOT) whereas 102 patients had no viral load measurements at 12 weeks EOT. Among the patients with HCV RNA data post-EOT 12, 116 (92.8%) had sustained viral response (SVR). The prevalence of death and loss-to-follow up (LTFU) were (7.5%, 95% CI 1.7-4.1) and 67 (28.1%, 95% CI 22.3-33.9) translating into an incidence of 1.1 (95% CI 0.8-1.5) per 10,000 person days. Independent predictors of LTFU included the enrollment year (2020: aHR = 2.2, 95% CI 1-4.7; p value = 0.04); Hospital (Hospital B: aHR = 2.2, 95% CI 1-4.7; p value = 0.03) and the FIB-4 score (FIB-Score < 1.45: aHR = 3.7, 95% CI 1.2-11.5; p value = 0.02). The SVR rates achieved in this cohort were high. However, high LTFU and high mortality driven largely by late presentation and suboptimal population screening/case finding, were uncovered. These challenges can be addressed by test-and-treat programs that simultaneously prioritize programmatic screening, decentralization of care, and better patient tracking in the HCV care cascade.
撒哈拉以南非洲地区缺乏有关直接作用抗病毒药物(DAA)的实际使用情况和治疗效果的可靠数据。本研究提供了厄立特里亚 HCV 患者基于 DAA 的治疗效果、死亡率、失访率及相关因素的数据。本研究采用回顾性多中心观察性队列研究方法,在厄立特里亚阿斯马拉的两家三级医院进行。使用结构化清单从患者病历中收集数据。采用均值(±标准差(SD)、中位数(四分位距(IQR)、卡方检验(χ)、Kaplan-Meier 估计值和多变量 Cox 比例风险模型进行描述性和推断性统计分析。本研究共纳入 238 名中位年龄为 59 岁(IQR 50-69 岁)的患者。在接受治疗的 227 名患者中,125 名患者在治疗结束后 12 周进行了病毒载量检测,而 102 名患者在治疗结束后 12 周未进行病毒载量检测。在 HCV RNA 数据 post-EOT12 的患者中,116 名(92.8%)有持续病毒应答(SVR)。死亡率和失访率分别为(7.5%,95%CI 1.7-4.1)和 67 例(28.1%,95%CI 22.3-33.9),换算为每 10000 人天发生 1.1 例(95%CI 0.8-1.5)。失访的独立预测因素包括入组年份(2020 年:aHR=2.2,95%CI 1-4.7;p 值=0.04)、医院(B 医院:aHR=2.2,95%CI 1-4.7;p 值=0.03)和 FIB-4 评分(FIB-Score<1.45:aHR=3.7,95%CI 1.2-11.5;p 值=0.02)。本队列中达到的 SVR 率较高。然而,由于晚期就诊和人群筛查/病例发现不理想,发现了高失访率和高死亡率。这些挑战可以通过同时优先考虑方案筛查、护理去中心化和更好的 HCV 护理级联中的患者跟踪的检测和治疗方案来解决。