Department of Pediatrics, Landeskrankenhaus Bregenz, Bregenz, Austria.
Department of Pediatrics, Division of Pediatric Rheumatology and autoinflammation reference center Tuebingen (arcT), Tuebingen, Germany.
Arthritis Res Ther. 2023 Nov 28;25(1):228. doi: 10.1186/s13075-023-03195-4.
Chronic non-bacterial osteomyelitis (CNO) is an autoinflammatory bone-disease of unknown origin. The National Pediatric Rheumatologic Database (NPRD) collects long-term data of children and adolescents with rheumatic diseases including CNO.
To assess characteristics, courses, and outcomes of CNO with onset in childhood and adolescence and to identify outcome predictors.
From 2015 to 2021 patients with a confirmed diagnosis of CNO, who were registered in the NPRD during their first year of disease and at least one follow-up visit, were included in this analysis and observed for up to 4 years.
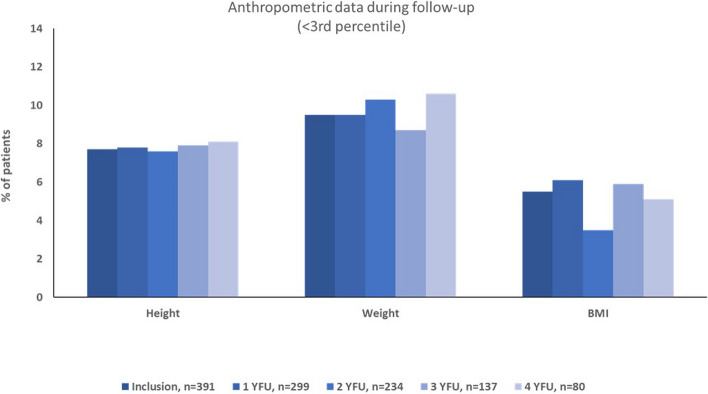
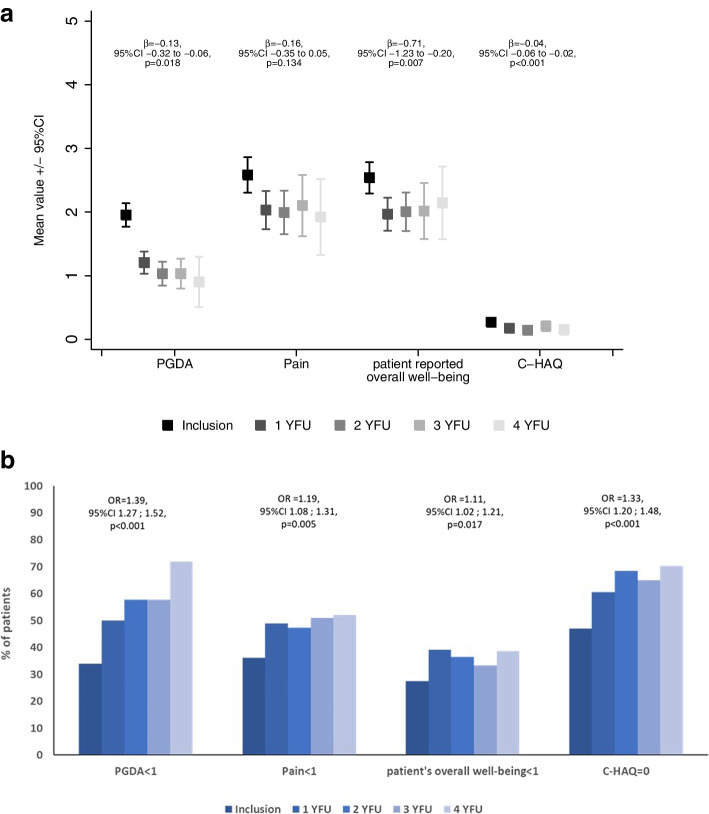
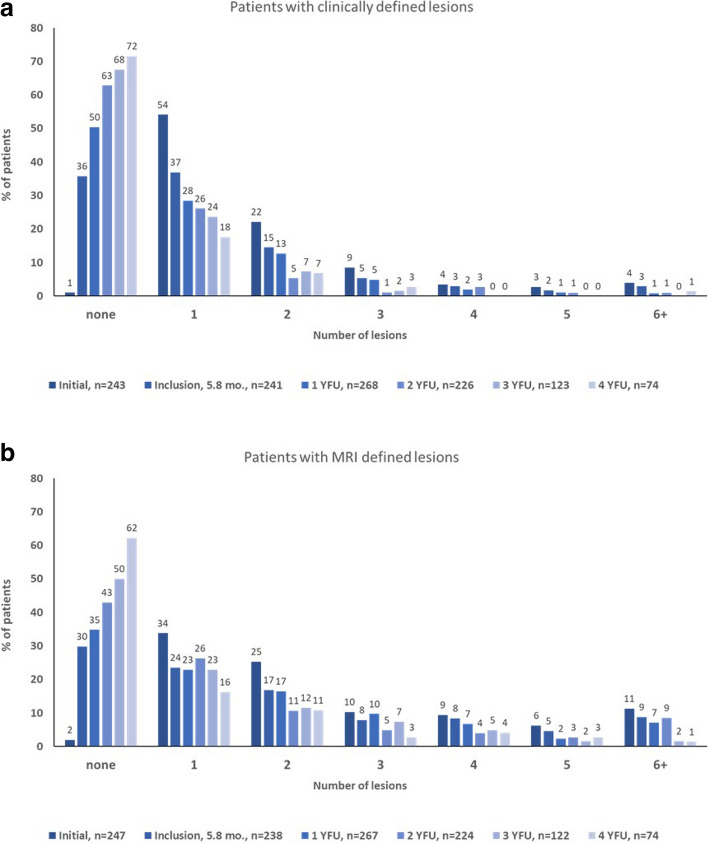
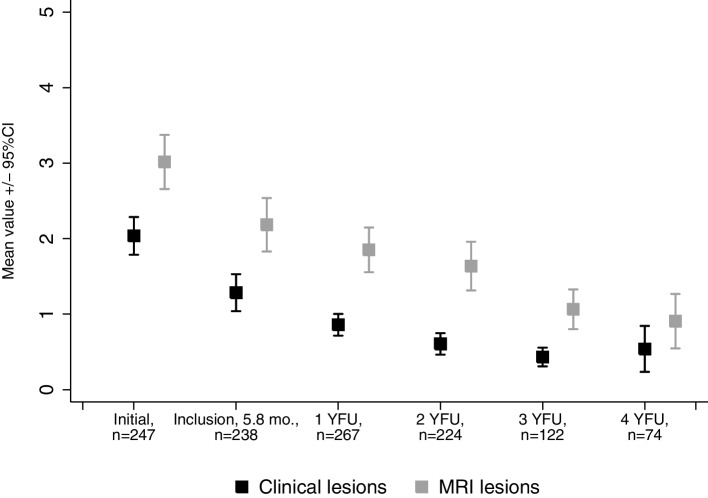
Four hundred patients with recent diagnosis of CNO were enrolled in the NRPD during the study period. After 4 years, patient data documentation was sufficient to be analyzed in 81 patients. A significant decline of clinical and radiological lesions is reported: at inclusion in the registry, the mean number of clinical lesions was 2.0 and 3.0 MRI lesions per patient. A significant decrease of manifestations during 4 years of follow-up (mean clinical lesions 0.5, p < 0.001; mean MRI lesions 0.9 (p < 0.001)) was documented. A significant improvement of physician global disease activity (PGDA), patient-reported overall well-being, and childhood health assessment questionnaire (C-HAQ) was documented. Therapeutically, an increase of disease-modifying anti-rheumatic drugs over the years can be stated, while bisphosphonates rather seem to be considered as a therapeutic DMARD option in the first years of disease. Only 5-7% of the patients had a severe disease course as defined by a PGDA > = 4. Predictors associated with a severe disease course include the site of inflammation (pelvis, lower extremity, clavicle), increased erythrocyte sedimentation rate, and multifocal disease at first documentation. The previously published composite PedCNO disease activity score was analyzed revealing a PedCNO70 in 55% of the patients at 4YFU.
An improvement of physician global disease activity (PGDA), patient reported overall well-being and imaging-defined disease activity measures was documented, suggesting that inactivity of CNO disease can be reached. PedCNO score and especially PGDA, MRI-defined lesions and in a number of patients also the C-HAQ seem to be reliable parameters for describing disease activity. The identification of risk factors at the beginning of the disease might influence treatment decision in the future.
慢性非细菌性骨髓炎(CNO)是一种病因不明的自身炎症性骨病。国家儿科风湿病数据库(NPRD)收集了包括 CNO 在内的儿童和青少年风湿病患者的长期数据。
评估儿童和青少年发病的 CNO 的特征、病程和结局,并确定结局预测因素。
本研究纳入了 2015 年至 2021 年期间在 NPRD 登记的、在疾病发病后第一年及至少一次随访时确诊为 CNO 的患者,并对其进行了长达 4 年的观察。
在研究期间,有 400 例 CNO 初诊患者在 NPRD 登记。4 年后,有 81 例患者的数据记录足以进行分析。研究结果显示,患者的临床和影像学病变显著改善:在登记时,每位患者的平均临床病变数为 2.0 个,MRI 病变数为 3.0 个。在 4 年的随访过程中,临床表现显著减少(平均临床病变数 0.5,p<0.001;平均 MRI 病变数 0.9(p<0.001))。研究还发现,医生总体疾病活动度(PGDA)、患者报告的整体健康状况和儿童健康评估问卷(C-HAQ)显著改善。治疗上,随着时间的推移,疾病修饰抗风湿药物的使用有所增加,而双膦酸盐似乎在疾病的最初几年被认为是一种治疗 DMARD 的选择。仅有 5-7%的患者出现了严重的疾病过程,定义为 PGDA≥4。与严重疾病过程相关的预测因素包括炎症部位(骨盆、下肢、锁骨)、红细胞沉降率升高和首次记录时多发病灶。研究还对之前发表的复合 PedCNO 疾病活动评分进行了分析,结果显示,4 年随访时,55%的患者达到了 PedCNO70。
研究结果表明,医生总体疾病活动度(PGDA)、患者报告的整体健康状况和影像学定义的疾病活动测量值得到了改善,这表明 CNO 疾病可能处于静止状态。PedCNO 评分,尤其是 PGDA、MRI 定义的病变以及在许多患者中,C-HAQ 似乎是描述疾病活动度的可靠参数。在疾病开始时识别出危险因素可能会影响未来的治疗决策。