Hansen Malene Kærslund, Mortensen Martin Bødtker, Warnakula Olesen Kevin Kris, Thrane Pernille Gro, Maeng Michael
Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark.
Department of Clinical Medicine, Health, Aarhus University, Aarhus, Denmark.
Lancet Reg Health Eur. 2023 Nov 4;36:100774. doi: 10.1016/j.lanepe.2023.100774. eCollection 2024 Jan.
Identifying patients at high residual risk of atherosclerotic cardiovascular disease (ASCVD) despite statin-treatment is of paramount clinical importance. We aim to investigate if non-high-density lipoprotein cholesterol (non-HDL-C) identifies residual risk of ASCVD and death in statin-treated patients with ischemic heart disease and low-density lipoprotein cholesterol (LDL-C) ≤ 1.8 mmol/L.
Leveraging Danish regional and national registries, we identified statin-treated patients with ischemic heart disease who underwent coronary angiography (CAG) and attained LDL-C ≤ 1.8 mmol/L within a year post-CAG. Outcomes were myocardial infarction (MI), ASCVD (MI or ischemic stroke), and all-cause death occurring from one year after CAG to end of follow-up. Cox regression analyses obtained adjusted hazard ratios (HR).
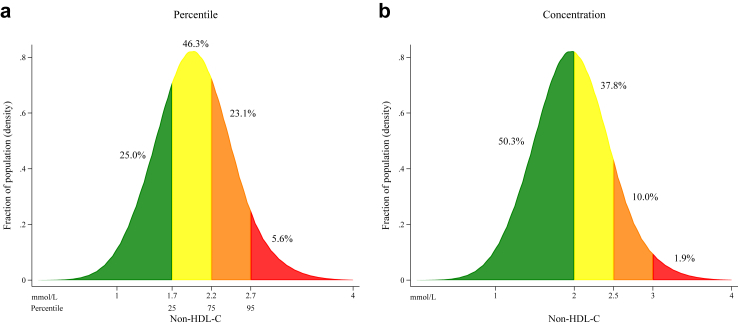
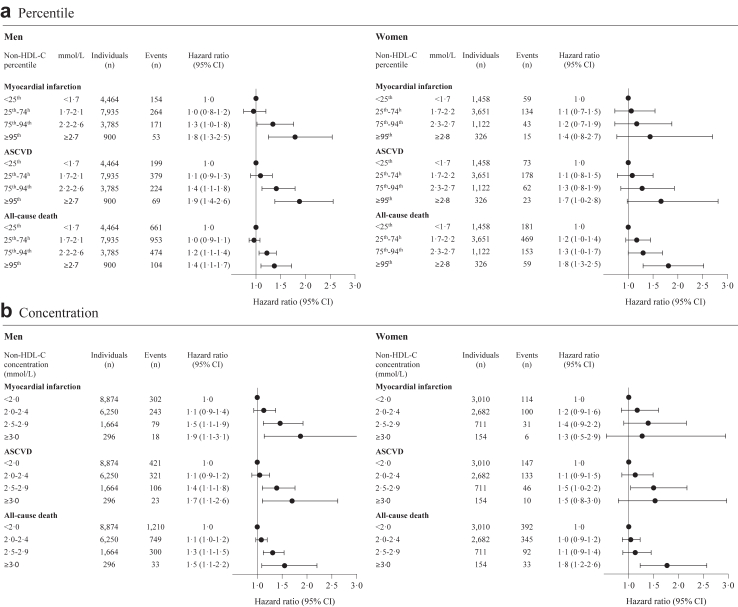
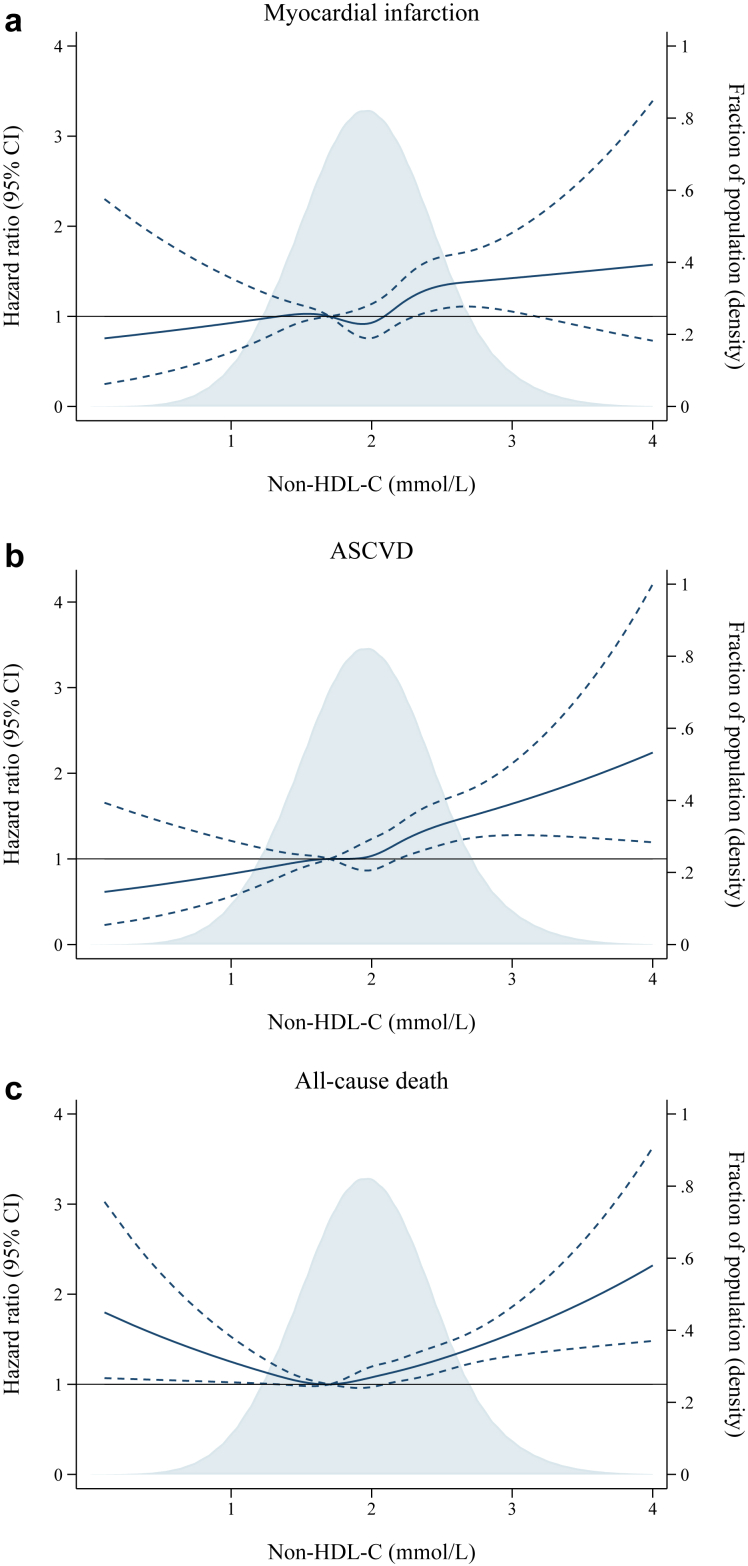
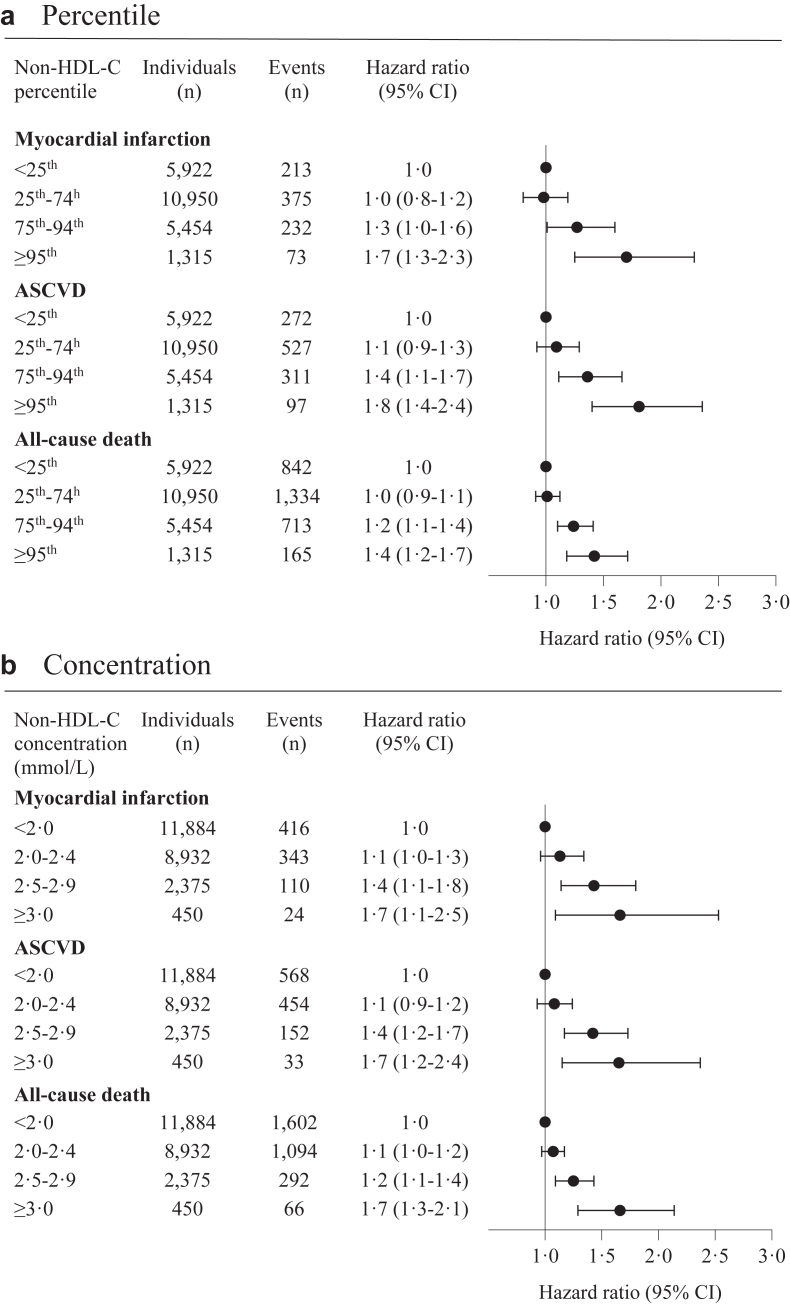
Between January 1, 2011, and December 31, 2020, we included 23,641 statin-treated patients with ischemic heart disease and LDL-C ≤ 1.8 mmol/L. During median follow-up of 4.1 years (IQR 2.4-6.1), 893 (3.8%) patients developed MI, 1207 (5.1%) ASCVD, and 3054 (12.9%) patients died. For ASCVD the adjusted HRs (95% confidence interval) for non-HDL-C < 25th percentile (<1.7 mmol/L) versus 25th-74th (1.7-2.1 mmol/L), 75th-94th (2.2-2.6 mmol/L), and ≥95th (≥2.7 mmol/L) percentile were 1.1 (0.9-1.3), 1.4 (1.1-1.7), and 1.8 (1.4-2.4), and for all-cause death 1.0 (0.9-1.1), 1.2 (1.1-1.4), and 1.4 (1.2-1.7), respectively.
In a contemporary secondary prevention cohort of patients with well-managed LDL-C, non-HDL-C emerges as an easily accessible marker to detect patients facing high residual risk of ASCVD and death. These findings are important for preventive strategies extending beyond LDL-C targets.
Research grant from the Novo Nordisk Foundation.
识别尽管接受了他汀类药物治疗但仍有动脉粥样硬化性心血管疾病(ASCVD)高残留风险的患者具有至关重要的临床意义。我们旨在研究非高密度脂蛋白胆固醇(non-HDL-C)是否能识别接受他汀类药物治疗的缺血性心脏病且低密度脂蛋白胆固醇(LDL-C)≤1.8 mmol/L患者的ASCVD和死亡残留风险。
利用丹麦地区和国家登记处的数据,我们识别出接受他汀类药物治疗的缺血性心脏病患者,这些患者接受了冠状动脉造影(CAG),并在CAG后一年内实现LDL-C≤1.8 mmol/L。结局指标为心肌梗死(MI)、ASCVD(MI或缺血性卒中)以及从CAG后一年至随访结束时发生的全因死亡。Cox回归分析得出调整后的风险比(HR)。
在2011年1月1日至2020年12月31日期间,我们纳入了23,641例接受他汀类药物治疗的缺血性心脏病且LDL-C≤1.8 mmol/L的患者。在中位随访4.1年(四分位间距2.4 - 6.1年)期间,893例(3.8%)患者发生MI,1207例(5.1%)发生ASCVD,3054例(12.9%)患者死亡。对于ASCVD,non-HDL-C处于第25百分位数以下(<1.7 mmol/L)与处于第25 - 74百分位数(1.7 - 2.1 mmol/L)、第75 - 94百分位数(2.2 - 2.6 mmol/L)以及≥第95百分位数(≥2.7 mmol/L)相比,调整后的HR(95%置信区间)分别为1.1(0.9 - 1.3)、1.4(1.1 - 1.7)和1.8(1.4 - 2.4),对于全因死亡分别为1.0(0.9 - 1.1)、1.2(1.1 - 1.4)和1.4(1.2 - 1.7)。
在一个当代LDL-C管理良好的患者二级预防队列中,non-HDL-C成为一种易于获取的标志物,可用于检测面临ASCVD和死亡高残留风险的患者。这些发现对于超出LDL-C目标的预防策略具有重要意义。
来自诺和诺德基金会的研究资助。