Infectious Diseases Institute, Makerere University College of Health Sciences, Kampala, Uganda.
Division of Infectious Diseases and International Medicine, Department of Medicine, University of Minnesota, Minneapolis, Minnesota, United States of America.
PLoS One. 2023 Nov 30;18(11):e0291834. doi: 10.1371/journal.pone.0291834. eCollection 2023.
Interferon-gamma release assay and tuberculin skin test use is limited by costly sundries and cross-reactivity with non-tuberculous mycobacteria and Bacille Calmette-Guérin (BCG) vaccination respectively. We investigated the Monocyte to Lymphocyte ratio (MLR) as a biomarker to overcome these limitations and for use in monitoring response to tuberculosis preventive therapy (TPT).
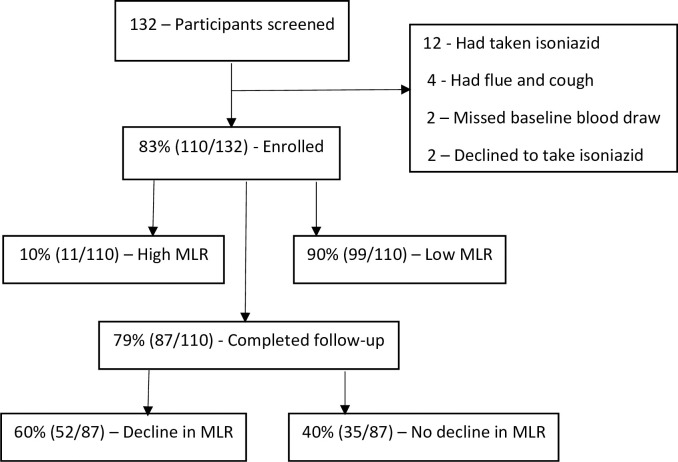
We conducted a cross-sectional and nested prospective observational study among asymptomatic adults living with Human Immuno-deficiency Virus (HIV) in Kampala, Uganda. Complete blood count (CBC) and QuantiFERON-TB® Gold-plus were measured at baseline and CBC repeated at three months. Multivariable logistic regression was performed to identify factors associated with a high MLR and decline in MLR.
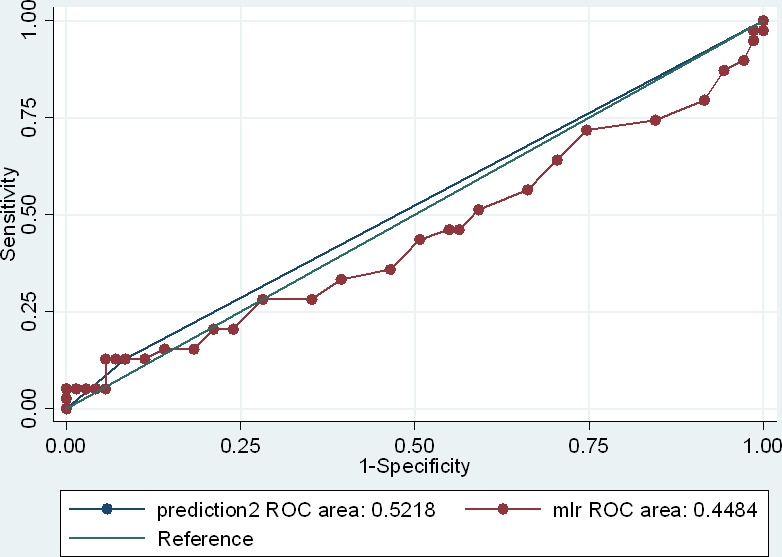
We recruited 110 adults living with HIV and on antiretroviral therapy, of which 82.5% (85/110) had suppressed viral loads, 71.8% (79/110) were female, and 73.6% (81/110) had a BCG scar. The derived MLR diagnostic cut-off was 0.35, based on which the MLR sensitivity, specificity, positive predictive value, and negative predictive value were 12.8%, 91.6%, 45.5%, and 65.7% respectively. The average MLR declined from 0.212 (95% CI: 0.190-0.235) at baseline to 0.182 (95% CI: 0.166-0.198) after three months of TPT. A viral load of >50 copies/ml (aOR, 5.67 [1.12-28.60]) was associated with a high MLR while that of <50 copies/ml (aOR, 0.07 [0.007-0.832]) was associated with a decline in MLR.
MLR was highly specific in diagnosing latent TB and declined significantly following three months of TPT. Implications of a high MLR and decline in MLR after TPT need further evaluation in a larger cohort.
干扰素-γ释放试验和结核菌素皮肤试验的使用分别受到昂贵耗材和与非结核分枝杆菌及卡介苗(BCG)疫苗交叉反应的限制。我们研究了单核细胞与淋巴细胞比值(MLR)作为一种生物标志物,以克服这些限制,并用于监测结核病预防治疗(TPT)的反应。
我们在乌干达坎帕拉对无症状的艾滋病毒感染者进行了横断面和嵌套前瞻性观察性研究。在基线时测量全血细胞计数(CBC)和 QuantiFERON-TB® Gold-plus,并在三个月时重复 CBC。进行多变量逻辑回归以确定与高 MLR 和 MLR 下降相关的因素。
我们招募了 110 名接受抗逆转录病毒治疗的艾滋病毒感染者,其中 82.5%(85/110)病毒载量得到抑制,71.8%(79/110)为女性,73.6%(81/110)有 BCG 疤痕。基于此,MLR 的诊断截止值为 0.35,其敏感性、特异性、阳性预测值和阴性预测值分别为 12.8%、91.6%、45.5%和 65.7%。在 TPT 三个月后,平均 MLR 从基线时的 0.212(95%CI:0.190-0.235)下降至 0.182(95%CI:0.166-0.198)。病毒载量>50 拷贝/ml(比值比,5.67 [1.12-28.60])与高 MLR 相关,而病毒载量<50 拷贝/ml(比值比,0.07 [0.007-0.832])与 MLR 下降相关。
MLR 在诊断潜伏性结核病方面具有高度特异性,并且在 TPT 三个月后显著下降。TPT 后 MLR 升高和下降的意义需要在更大的队列中进一步评估。