UConn Health, Center on Aging, Farmington, Connecticut.
Connecticut Department of Social Services, Hartford, Connecticut.
JAMA Health Forum. 2023 Dec 1;4(12):e234240. doi: 10.1001/jamahealthforum.2023.4240.
Hospice care enhances quality of life for people with terminal illness and is most beneficial with longer length of stay (LOS). Most hospice research focuses on the Medicare-insured population. Little is known about hospice use for the racially and ethnically diverse, low-income Medicaid population.
To compare hospice use and hospice LOS by race and ethnicity among Medicaid-only individuals and those with dual eligibility for Medicare and Medicaid (duals) in the Connecticut Medicaid program who died over a 4-year period.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective population-based cohort study used Medicaid and traditional Medicare enrollment and claims data for 2015 to 2020. The study included Connecticut Medicaid recipients with at least 1 of 5 most common hospice diagnoses who died from 2017 to 2020.
Race and ethnicity.
Hospice use (yes/no) and hospice LOS (1-7 days vs ≥8 days.) Covariates included sex, age, and nursing facility stay within 60 days of death.
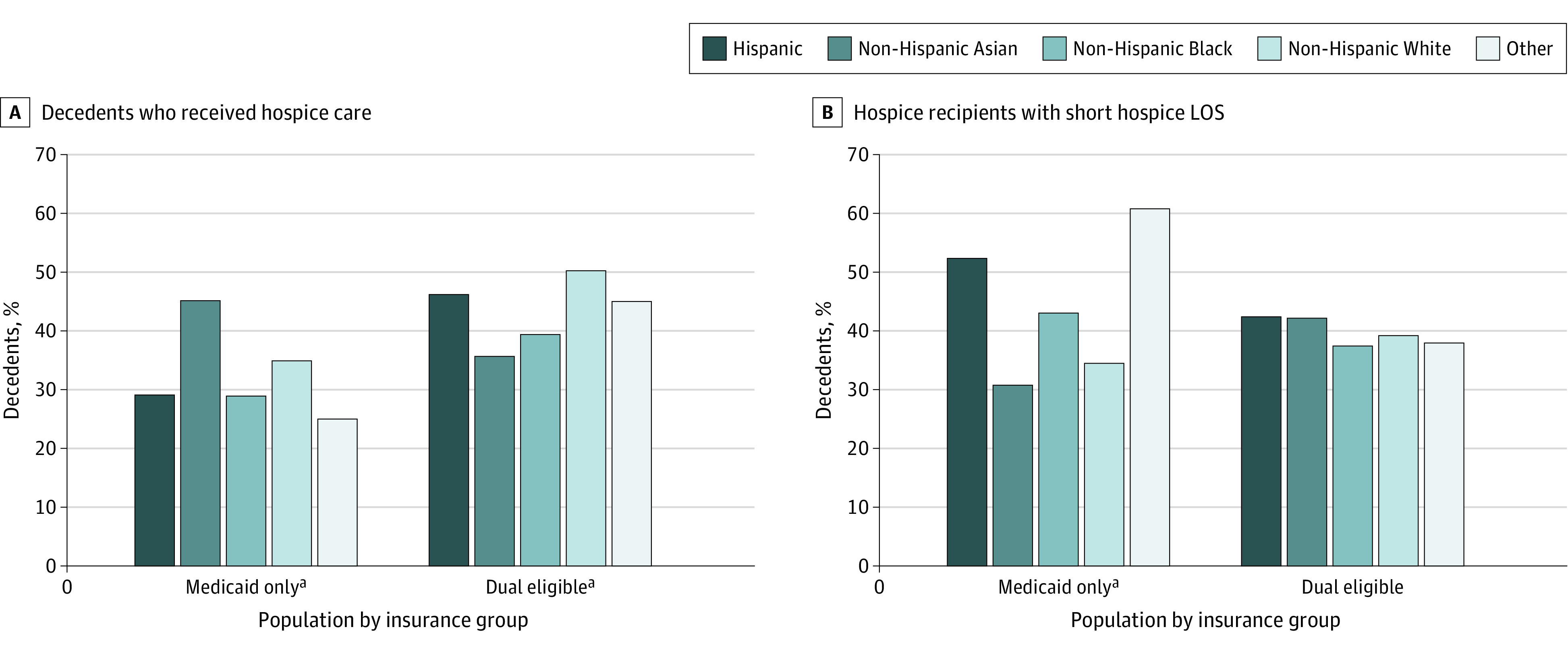
Overall, 2407 and 23 857 duals were included. Medicaid-only decedents were younger (13.8% ≥85 vs 52.5%), more likely to be male (50.6% vs 36.4%), more racially and ethnically diverse (48.7% non-Hispanic White vs 79.9%), and less likely to have a nursing facility stay (34.9% vs 56.1%). Race and ethnicity were significantly associated with hospice use and LOS in both populations: non-Hispanic Black and Hispanic decedents had lower odds of using hospice than non-Hispanic White decedents, and Hispanic decedents had higher odds of a short LOS. In both populations, older age and female sex were also associated with more hospice use. For duals only, higher age was associated with lower odds of short LOS. For decedents with nursing facility stays, compared with those without, Medicaid-only decedents had higher odds of using hospice (odds ratio [OR], 1.49; 95% CI, 1.24-1.78); duals had lower odds (OR, 0.60; 95% CI, 0.57-0.63). Compared with decedents without nursing facility stays, duals with a nursing facility stay had higher odds of short LOS (OR, 2.63; 95% CI, 2.43-2.85).
Findings raise concerns about equity and timing of access to hospice for Hispanic and non-Hispanic Black individuals in these understudied Medicaid populations. Knowledge about, access to, and acceptance of hospice may be lacking for these low-income individuals. Further research is needed to understand barriers to and facilitators of hospice use for people with nursing facility stays.
临终关怀可提高绝症患者的生活质量,且入住时间(LOS)越长越有益。大多数临终关怀研究都集中在有医疗保险的人群上。对于种族和民族多样化、低收入的医疗补助人群,临终关怀的使用情况知之甚少。
在康涅狄格州医疗补助计划中,比较仅接受医疗补助和同时有医疗保险和医疗补助资格(双重资格)的个人在四年期间的种族和民族之间的临终关怀使用情况和临终关怀 LOS。
设计、地点和参与者:这是一项回顾性基于人群的队列研究,使用了 2015 年至 2020 年的医疗补助和传统医疗保险登记和索赔数据。研究纳入了至少有 5 种最常见临终关怀诊断之一的康涅狄格州医疗补助受助人,这些受助人在 2017 年至 2020 年期间死亡。
种族和民族。
临终关怀的使用(是/否)和临终关怀 LOS(1-7 天与≥8 天)。协变量包括性别、年龄和死亡前 60 天内的护理院停留情况。
总体而言,纳入了 2407 名双重资格和 23857 名仅接受医疗补助的死者。仅接受医疗补助的死者年龄更小(13.8%≥85 岁 vs 52.5%),更可能为男性(50.6% vs 36.4%),种族和民族更为多样化(48.7%非西班牙裔白人 vs 79.9%),且护理院停留的可能性更小(34.9% vs 56.1%)。在两个群体中,种族和民族与临终关怀的使用和 LOS 显著相关:非西班牙裔黑人死者和西班牙裔死者使用临终关怀的可能性低于非西班牙裔白人死者,而西班牙裔死者的 LOS 较短。在两个群体中,年龄较大和女性也与更多的临终关怀使用相关。仅对双重资格者而言,年龄较大与较短 LOS 的可能性降低相关。对于有护理院停留的死者,与没有护理院停留的死者相比,仅接受医疗补助的死者使用临终关怀的可能性更高(优势比 [OR],1.49;95%CI,1.24-1.78);双重资格者的可能性较低(OR,0.60;95%CI,0.57-0.63)。与没有护理院停留的死者相比,有护理院停留的双重资格者 LOS 较短的可能性更高(OR,2.63;95%CI,2.43-2.85)。
研究结果令人担忧,在这些研究较少的医疗补助人群中,西班牙裔和非西班牙裔黑人个人获得临终关怀的机会和时间存在公平性问题。这些低收入人群可能对临终关怀的了解、获得和接受程度较低。需要进一步研究以了解有护理院停留的人使用临终关怀的障碍和促进因素。