Division of Surgery and Oncology, Department of Clinical Science Intervention and Technology (CLINTEC) Karolinska Institutet, and Department of Upper Abdominal Diseases, Karolinska University Hospital, Stockholm, Sweden.
Division of Ear, Nose and Throat Diseases, Department of Clinical Science Intervention and Technology (CLINTEC) Karolinska Institutet, and Department of Ear, Nose and Throat Diseases, Karolinska University Hospital, Stockholm, Sweden.
Dis Esophagus. 2024 Feb 29;37(3). doi: 10.1093/dote/doad068.
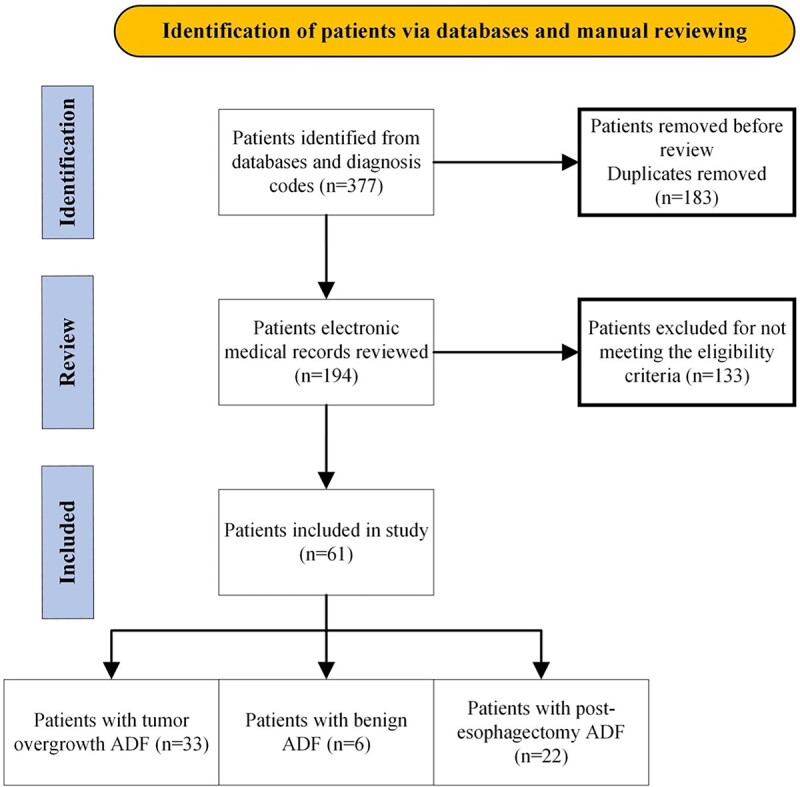
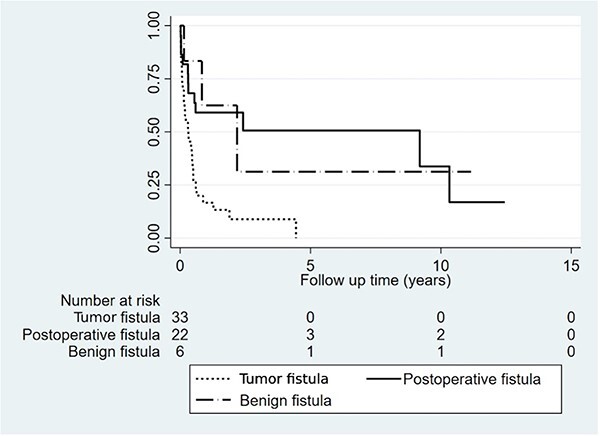
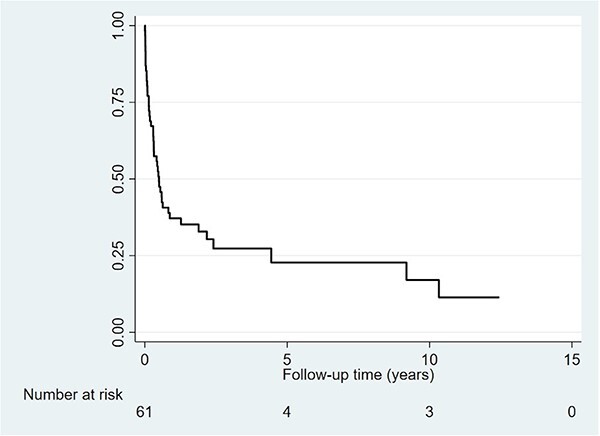
Aerodigestive fistula (ADF) is defined as a pathological connection between the upper digestive tract and the airway. ADF is associated with high morbidity and mortality and management is often complex. A cohort study including all patients admitted with ADF 2004-2022 at a single tertiary esophageal surgery center was performed based on prospectively collected administrative data and retrospectively collected electronic patient chart data,. Patient demographics, performance status, comorbidity, fistula characteristics, management, and outcomes in terms of morbidity and mortality were assessed in patients with ADF of three distinct types: (i) tumor overgrowth-related, (ii) various benign etiologies, and (iii) post-esophagectomy. Sixty-one patients with ADF were included in the study, 33 (54.1%) tumor overgrowth-related, six (9.8%) benign and 22 (36.1%) post-esophagectomy. In the post-esophagectomy group 15 out of 22 (68.2%) patients were diagnosed with anastomotic leakage prior to ADF diagnosis. Self-expandable metallic stents (SEMS) were used for temporary fistula sealing in 59 out of 61 (96.7%) patients, of which most received stents in both the digestive tract and airway. Temporary fistula sealing with stents was successful enabling discharge from hospital in 47 out of 59 (79.7%) patients. Definitive ADF repair was performed in 16 (26.2%) patients, of which one (6.3%) died within 90-days and 15 could be discharged home with permanently sealed fistulas. ADF is a complex condition associated with high mortality, which often requires multiple advanced interventions. SEMS can be applied in the airway and simultaneously in the digestive tract to temporarily seal the ADF as bridge to definitive surgical repair.
气道-消化瘘(ADF)是指上消化道与气道之间病理性的连通。ADF 与高发病率和高死亡率相关,其治疗通常较为复杂。本研究基于前瞻性收集的行政数据和回顾性收集的电子患者病历数据,对 2004 年至 2022 年期间在一家单一的三级食管外科中心因 ADF 入院的所有患者进行了一项队列研究。研究评估了 ADF 三种不同类型患者的人口统计学特征、功能状态、合并症、瘘管特征、管理以及发病率和死亡率相关的结局:(i)肿瘤过度生长相关、(ii)各种良性病因和(iii)食管切除术后。研究共纳入 61 例 ADF 患者,其中 33 例(54.1%)与肿瘤过度生长相关,6 例(9.8%)为良性病因,22 例(36.1%)为食管切除术后。在食管切除术后组中,22 例患者中有 15 例(68.2%)在 ADF 诊断前被诊断为吻合口漏。59 例(96.7%)患者中使用了自膨式金属支架(SEMS)进行暂时性瘘管封堵,其中大多数患者的消化道和气道中均放置了支架。通过支架进行的暂时性瘘管封堵有 47 例(79.7%)患者成功封堵瘘管并出院。16 例(26.2%)患者进行了 ADF 确定性修复,其中 1 例(6.3%)在 90 天内死亡,15 例患者能够出院回家,瘘管永久性封堵。ADF 是一种复杂的疾病,死亡率高,往往需要多次高级干预。SEMS 可同时应用于气道和消化道,暂时封堵 ADF,作为确定性手术修复的桥梁。