San Mateo Division, Anesthesia Care Associates Medical Group (ACAMG), San Mateo, CA, 94010, USA.
Department of Anesthesia and Perioperative Care, Division of Critical Care Medicine, University of California, San Francisco, San Francisco, CA, USA.
Can J Anaesth. 2024 Jan;71(1):55-65. doi: 10.1007/s12630-023-02639-4. Epub 2023 Dec 15.
We sought to evaluate the synergistic risk of postoperative thrombosis in patients with a history of COVID-19 who undergo major surgery. Major surgery and SARS-CoV-2 infection are independently associated with an increased risk of thrombosis, but the magnitude of additional risk beyond surgery conferred by a COVID-19 history on the development of perioperative thrombotic events has not been clearly elucidated in the literature.
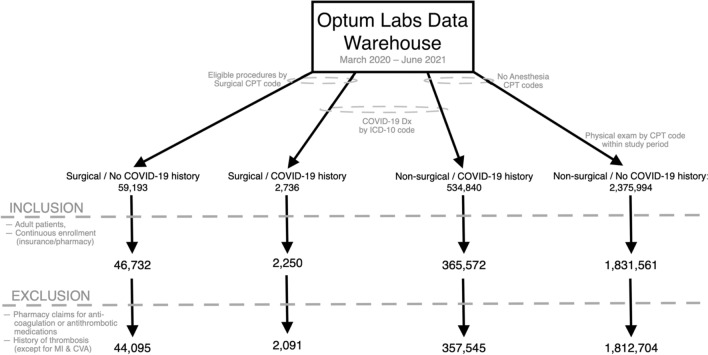
We conducted a retrospective cohort study among commercially insured adults in the USA from March 2020 to June 2021 using the Optum Labs Data Warehouse (OLDW), a longitudinal, real-world data asset containing deidentified administrative claims and electronic health records. We compared patients with prior COVID-19 who underwent surgery with control individuals who underwent surgery without a COVID-19 history and with control individuals who did not undergo surgery with and without a COVID-19 history. We assessed the interaction of surgery and previous COVID-19 on perioperative thrombotic events (venous thromboembolism and major adverse cardiovascular events) within 90 days using multivariable logistic regression and interaction analysis.
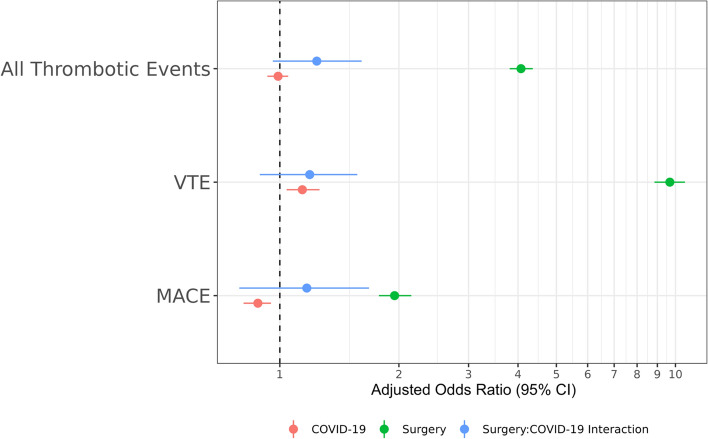
Two million and two-hundred thousand eligible patients were identified from the OLDW. Patients in the surgical cohorts were older and more medically complex than nonsurgical population controls. After adjusting for confounders, only surgical exposure-not COVID-19 history-remained associated with perioperative thrombotic events (adjusted odds ratio [aOR], 4.07; 95% confidence interval [CI], 3.81 to 4.36). The multiplicative interaction term (aOR, 1.25; 95% CI, 0.96 to 1.61) and the synergy index (0.76; 95% CI, 0.56 to 1.04) suggest minimal effect modification of prior COVID-19 on surgery with regards to overall thrombotic risk.
We found no evidence of synergistic thrombotic risk from previous COVID-19 in patients who underwent selected major surgery relative to the baseline thrombotic risk from surgery alone.
我们旨在评估有 COVID-19 病史的患者在接受重大手术后发生术后血栓形成的协同风险。重大手术和 SARS-CoV-2 感染均与血栓形成风险增加独立相关,但 COVID-19 病史对围手术期血栓形成事件发生的额外风险程度,在文献中尚未明确阐明。
我们在美国使用 Optum Labs 数据仓库(OLDW)进行了一项回顾性队列研究,该数据库是一个包含去标识化行政索赔和电子健康记录的纵向真实世界数据资产。我们比较了有 COVID-19 病史并接受手术的患者与接受手术且无 COVID-19 病史的患者,以及既未接受手术也无 COVID-19 病史的患者。我们使用多变量逻辑回归和交互分析评估手术和既往 COVID-19 对术后 90 天内围手术期血栓形成事件(静脉血栓栓塞和主要不良心血管事件)的交互作用。
从 OLDW 中确定了 220 万名符合条件的患者。手术队列中的患者比非手术人群对照组年龄更大,且病情更复杂。调整混杂因素后,只有手术暴露(而非 COVID-19 病史)与围手术期血栓形成事件相关(校正比值比 [aOR],4.07;95%置信区间 [CI],3.81 至 4.36)。乘法交互项(aOR,1.25;95%CI,0.96 至 1.61)和协同指数(0.76;95%CI,0.56 至 1.04)表明,既往 COVID-19 对手术总体血栓形成风险的影响轻微。
我们发现,与单独手术的基线血栓形成风险相比,既往 COVID-19 对接受某些重大手术的患者没有协同血栓形成风险。