University of L'Aquila, Department of Life, Health and Environmental Sciences; Internal Medicine and Nephrology Division, ASL 1 Avezzano-Sulmona-L'Aquila, San Salvatore Hospital, L'Aquila, Italy.
Anatomy and Pathological Histology Division, ASL 1 Avezzano-Sulmona-L'Aquila, San Salvatore Hospital, L'Aquila, Italy.
Medicine (Baltimore). 2023 Dec 15;102(50):e36560. doi: 10.1097/MD.0000000000036560.
Immune system deregulation, including AAV, is a key event that may potentially evolve into ESRD. Abnormal activation of the cAP is also a cardinal feature of TMA, particularly aHUS. The kidney is the most frequently involved organ, and renal-limited forms of TMA are often encountered in clinical practice. Isolated case reports described the occurrence of renal TMA in AAV patients. Some cases of both de novo and relapses of AAV and/or TMAs after anti-SARS-CoV2 vaccination have been reported. We reported, for the 1st time, a case of patients with new-onset MPA and aHUS occurring 3 weeks after the third dose of mRNA-1273 vaccine anti-SARS-CoV2.
We present a 67-year-old man, affected by arterial hypertension, reported, after mRNA-1273 vaccine anti-SARS-CoV2, anuria, fatigue, anorexia and nausea. Laboratory data revealed acute renal failure.
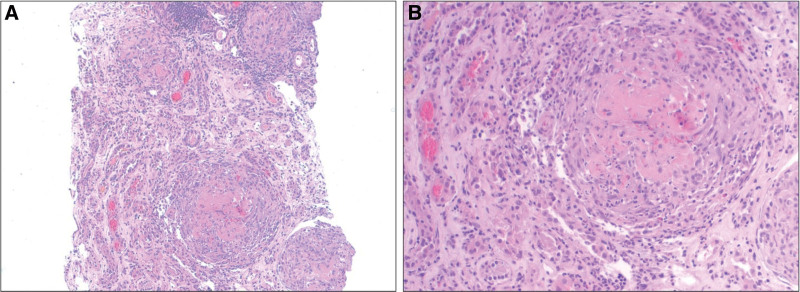
Positivity of MPO-ANCA was observed. 7 days after admission, we observed a worsening of anemia and thrombocytopenia with haptoglobin reduction, LDH increase and presence of schistocytes. Plasma levels of ADAMTS-13 were normal. A renal biopsy was performed, and findings were consistent with microscopic polyangiitis, with features of micro-thrombotic glomerulopathy. Genetic tests revealed absence of hybrid genes associated with the increased risk of aHUS.
We started renal replacement treatment, including hemodialysis, and pulsed methylprednisolone, with no improvement of laboratory parameters. Then, plasma exchange was performed leading to partial haematological response. Only with Eculizumab, a human C5 inhibitor, we observed a normalization of haptoglobin levels and platelets' count. However, three months after discharge, the patient still required hemodialysis.
To our knowledge we observed the first case aHUS, without genetic predisposition, associated with MPA occurring after the third dose of anti-SARS-CoV2 vaccine. This case report highlights the potential link between anti-SARS-CoV2 vaccine as a trigger of MPA and aHUS. This systematic review offers additional perspectives. It is plausible to hypothesize that the vaccine was the trigger for the development of these 2 diseases.Solid evidence on the mechanisms of interaction between vaccine and immune system, the role of genetic predisposition, and other variables, will shed additional light on the controversial link between anti-SARS-CoV2 vaccine and autoimmunity.
免疫系统失调,包括抗中性粒细胞胞浆抗体(antineutrophil cytoplasmic antibody,ANCA)相关性血管炎(antineutrophil cytoplasmic antibody–associated vasculitis,AAV),是可能发展为终末期肾脏疾病(end-stage renal disease,ESRD)的关键事件。补体激活异常也是血栓性微血管病(thrombotic microangiopathy,TMA)的主要特征,尤其是抗磷脂酶 A2 受体抗体(anti–phospholipase A2 receptor antibody,aPLA2R)相关性膜性肾病(membranous nephropathy,MN)。肾脏是最常受累的器官,临床上常遇到以肾脏受累为主的 TMA 形式。已有孤立病例报告描述了 AAV 患者发生肾 TMA 的情况。也有报道称,在接种抗严重急性呼吸综合征冠状病毒 2(severe acute respiratory syndrome coronavirus 2,SARS-CoV2)疫苗后,AAV 会出现新发或复发,包括 aHUS。我们首次报道了一例患者在接种第三剂 mRNA-1273 抗 SARS-CoV2 疫苗后 3 周出现新发性显微镜下多血管炎(microscopic polyangiitis,MPA)和 aHUS。
我们报告了一例 67 岁男性患者,有动脉高血压病史,在接种 mRNA-1273 抗 SARS-CoV2 疫苗后出现无尿、乏力、厌食和恶心。实验室数据显示急性肾衰竭。
抗髓过氧化物酶抗体(myeloperoxidase-antineutrophil cytoplasmic antibody,MPO-ANCA)阳性。入院后 7 天,患者出现贫血和血小板减少,伴触珠蛋白降低、乳酸脱氢酶(lactate dehydrogenase,LDH)升高和裂体细胞。ADAMTS-13 血浆水平正常。进行了肾活检,结果符合显微镜下多血管炎,伴有微血栓性肾小球病的特征。基因检测显示无与 aHUS 风险增加相关的杂合基因。
我们开始进行肾脏替代治疗,包括血液透析和脉冲甲基泼尼松龙,但实验室参数无改善。随后进行了血浆置换,使血液学指标部分恢复。仅用依库珠单抗(一种人 C5 抑制剂),我们观察到触珠蛋白水平和血小板计数恢复正常。然而,出院 3 个月后,患者仍需血液透析。
据我们所知,我们观察到首例无遗传易感性的抗 SARS-CoV2 疫苗接种后与 MPA 相关的 aHUS。本病例报告强调了抗 SARS-CoV2 疫苗作为 MPA 和 aHUS 发病诱因的潜在联系。本系统综述提供了更多的观点。推测疫苗可能是这些疾病发生的诱因。关于疫苗与免疫系统相互作用的机制、遗传易感性和其他变量的确凿证据将进一步阐明抗 SARS-CoV2 疫苗与自身免疫之间有争议的联系。