Division of HIV, Infectious Diseases, and Global Medicine, Department of Medicine, University of California San Francisco, San Francisco, CA, United States.
Université François Rabelais, Tours, France.
Front Cell Infect Microbiol. 2023 Dec 11;13:1297281. doi: 10.3389/fcimb.2023.1297281. eCollection 2023.
New drugs targeting antimicrobial resistant pathogens, including , have been challenging to evaluate in clinical trials, particularly for the non-ventilated hospital-acquired pneumonia and ventilator-associated pneumonia indications. Development of new antibacterial drugs is facilitated by preclinical animal models that could predict clinical efficacy in patients with these infections.
We report here an FDA-funded study to develop a rabbit model of non-ventilated pneumonia with by determining the extent to which the natural history of animal disease reproduced human pathophysiology and conducting validation studies to evaluate whether humanized dosing regimens of two antibiotics, meropenem and tobramycin, can halt or reverse disease progression.
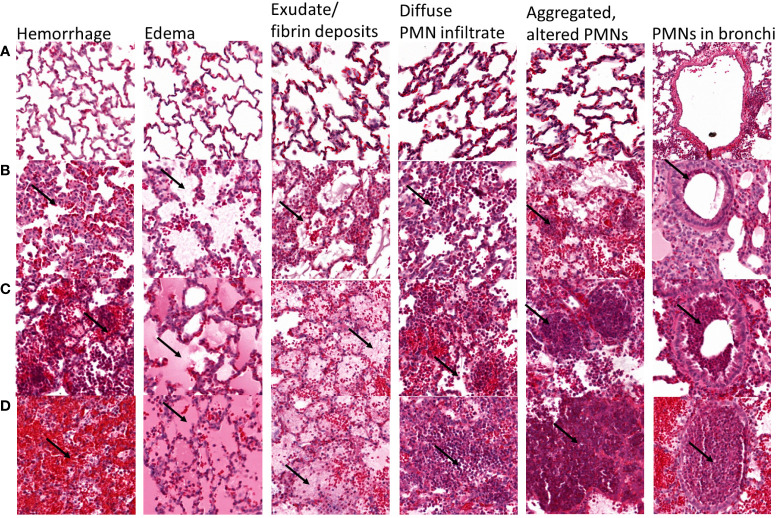
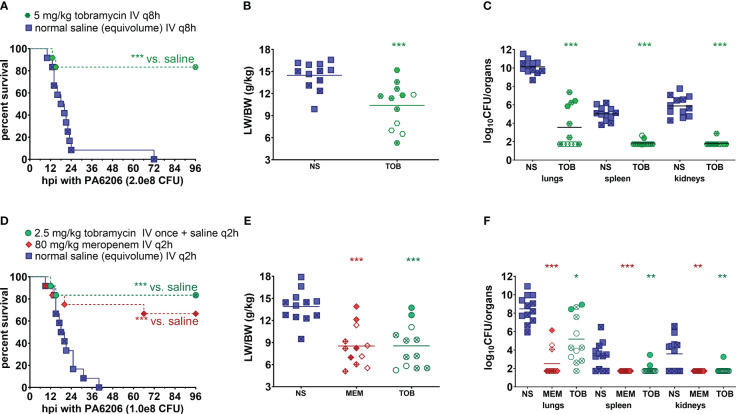
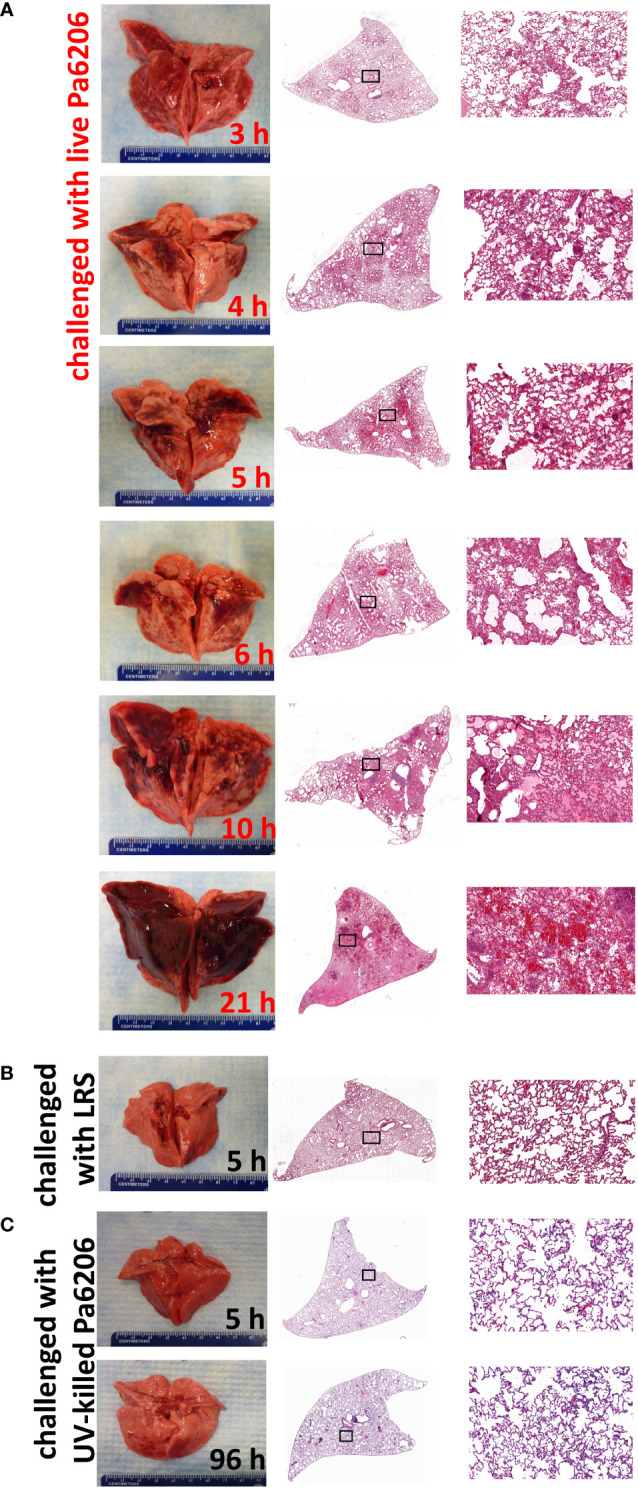
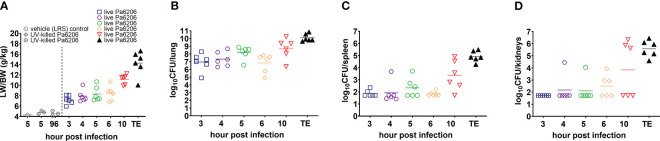
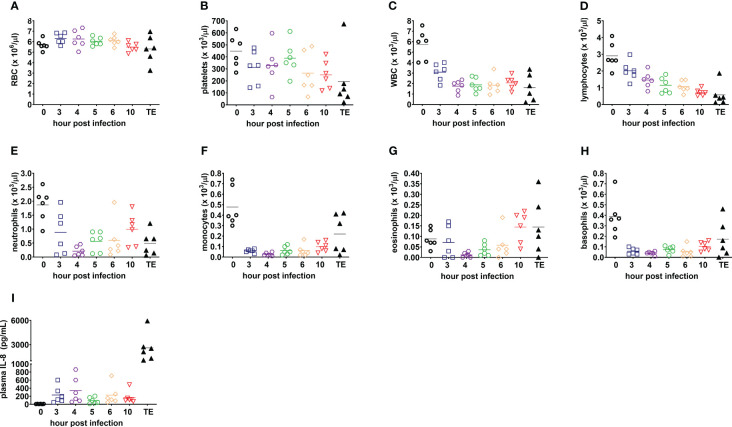
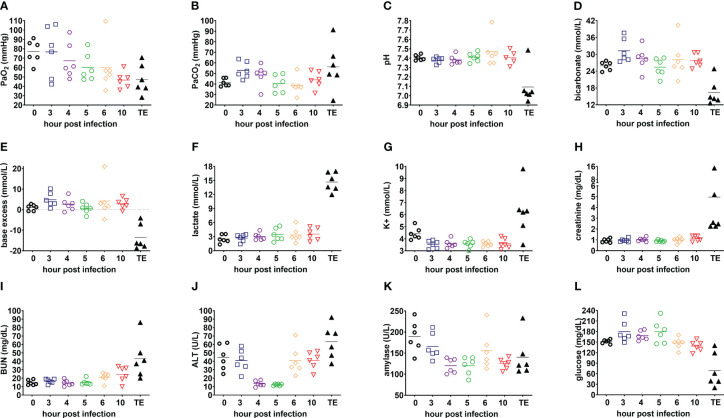
In a rabbit model of non-ventilated pneumonia, endobronchial challenge with live 6206, but not with UV-killed Pa6206, caused acute respiratory distress syndrome, as evidenced by acute lung inflammation, pulmonary edema, hemorrhage, severe hypoxemia, hyperlactatemia, neutropenia, thrombocytopenia, and hypoglycemia, which preceded respiratory failure and death. Pa6206 increased >100-fold in the lungs and then disseminated from there to infect distal organs, including spleen and kidneys. At 5 h post-infection, 67% of Pa6206-challenged rabbits had PaO <60 mmHg, corresponding to a clinical cut-off when oxygen therapy would be required. When administered at 5 h post-infection, humanized dosing regimens of tobramycin and meropenem reduced mortality to 17-33%, compared to 100% for saline-treated rabbits (<0.001 by log-rank tests). For meropenem which exhibits time-dependent bactericidal activity, rabbits treated with a humanized meropenem dosing regimen of 80 mg/kg q2h for 24 h achieved 100% T>MIC, resulting in 75% microbiological clearance rate of Pa6206 from the lungs. For tobramycin which exhibits concentration-dependent killing, rabbits treated with a humanized tobramycin dosing regimen of 8 mg/kg q8h for 24 h achieved C/MIC of 9.8 ± 1.4 at 60 min post-dose, resulting in 50% lung microbiological clearance rate. In contrast, rabbits treated with a single tobramycin dose of 2.5 mg/kg had C/MIC of 7.8 ± 0.8 and 8% (1/12) microbiological clearance rate, indicating that this rabbit model can detect dose-response effects.
The rabbit model may be used to help predict clinical efficacy of new antibacterial drugs for the treatment of non-ventilated pneumonia.
针对包括 在内的抗微生物药物耐药病原体的新药在临床试验中评估一直具有挑战性,尤其是在非呼吸机相关性医院获得性肺炎和呼吸机相关性肺炎的适应证中。临床前动物模型的发展有助于开发新的抗菌药物,这些模型可以预测这些感染患者的临床疗效。
我们在此报告了一项由美国食品和药物管理局资助的研究,该研究旨在通过确定动物疾病的自然史在多大程度上再现人类病理生理学,并进行验证研究以评估两种抗生素美罗培南和妥布霉素的人源化剂量方案是否可以阻止或逆转疾病进展,从而开发一种非呼吸机相关性肺炎的兔模型。
在非呼吸机相关性肺炎的兔模型中,用活的 6206 而不是用 UV 灭活的 Pa6206 经支气管内挑战会引起急性呼吸窘迫综合征,这表现为急性肺炎症、肺水肿、出血、严重低氧血症、高乳酸血症、中性粒细胞减少症、血小板减少症和低血糖症,这些都先于呼吸衰竭和死亡。Pa6206 在肺部中增加了 >100 倍,然后从那里传播到感染远端器官,包括脾脏和肾脏。在感染后 5 小时,67%的 Pa6206 感染兔的 PaO <60 mmHg,这相当于需要氧疗的临床截止值。当在感染后 5 小时给予时,妥布霉素和美罗培南的人源化剂量方案将死亡率降低至 17-33%,而生理盐水治疗的兔的死亡率为 100%(对数秩检验<0.001)。对于具有时间依赖性杀菌活性的美罗培南,接受人源化美罗培南剂量方案(80 mg/kg,q2h,共 24 小时)治疗的兔实现了 100%T>MIC,导致肺中 Pa6206 的微生物清除率为 75%。对于具有浓度依赖性杀菌作用的妥布霉素,接受人源化妥布霉素剂量方案(8 mg/kg,q8h,共 24 小时)治疗的兔在 60 分钟时达到 C/MIC 为 9.8±1.4,导致肺微生物清除率为 50%。相比之下,接受单次 2.5 mg/kg 妥布霉素治疗的兔的 C/MIC 为 7.8±0.8,微生物清除率为 8%(1/12),表明该兔模型可以检测剂量反应效应。
该兔模型可用于帮助预测新抗菌药物治疗非呼吸机相关性肺炎的临床疗效。