Ullah Anhar, Granell Raquel, Haider Sadia, Lowe Lesley, Fontanella Sara, Arshad Hasan, Murray Clare S, Turner Steve, Holloway John W, Simpson Angela, Roberts Graham, Custovic Adnan
National Heart and Lung Institute, Imperial College London, UK.
NIHR Imperial Biomedical Research Centre, London, UK.
EClinicalMedicine. 2023 Dec 12;67:102355. doi: 10.1016/j.eclinm.2023.102355. eCollection 2024 Jan.
Spirometric obstruction and restriction are two patterns of impaired lung function which are predictive of poor health. We investigated the development of these phenotypes and their transitions through childhood to early adulthood.
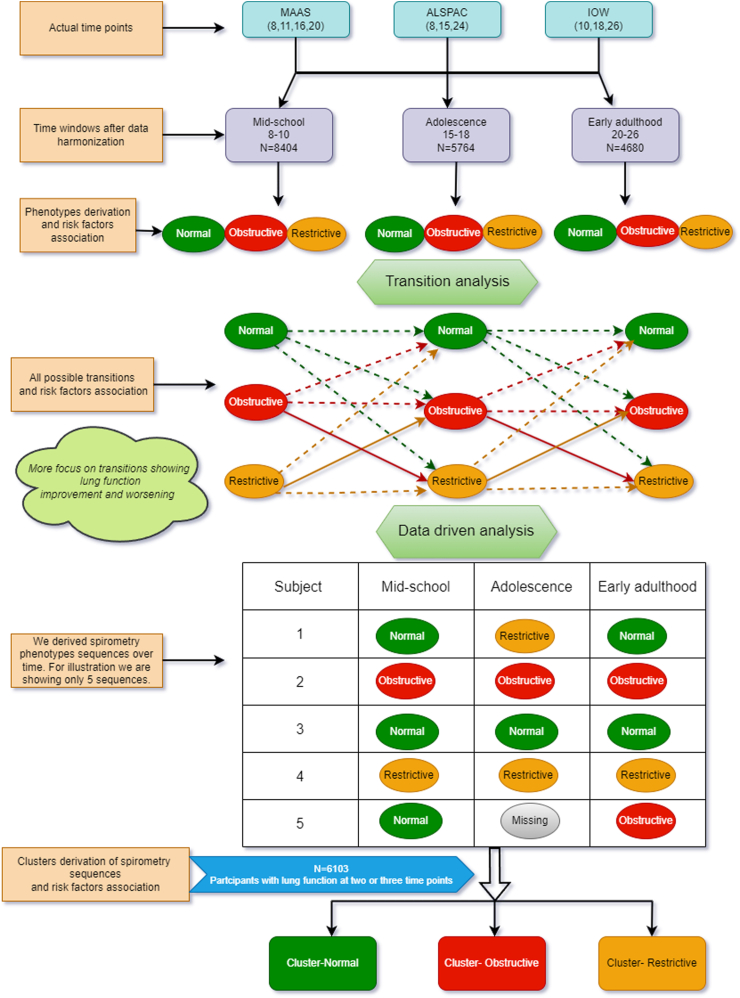
In this study, we analysed pooled data from three UK population-based birth cohorts established between 1989 and 1995. We applied descriptive statistics, regression modelling and data-driven modelling to data from three population-based birth cohorts with at least three spirometry measures from childhood to adulthood (mid-school: 8-10 years, n = 8404; adolescence: 15-18, n = 5764; and early adulthood: 20-26, n = 4680). Participants were assigned to normal, restrictive, and obstructive spirometry based on adjusted regression residuals. We considered two transitions: from 8-10 to 15-18 and from 15-18 to 20-26 years.
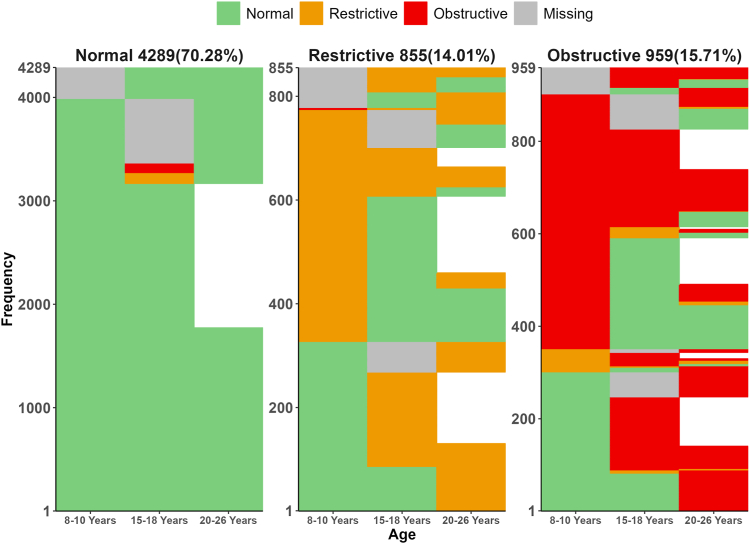
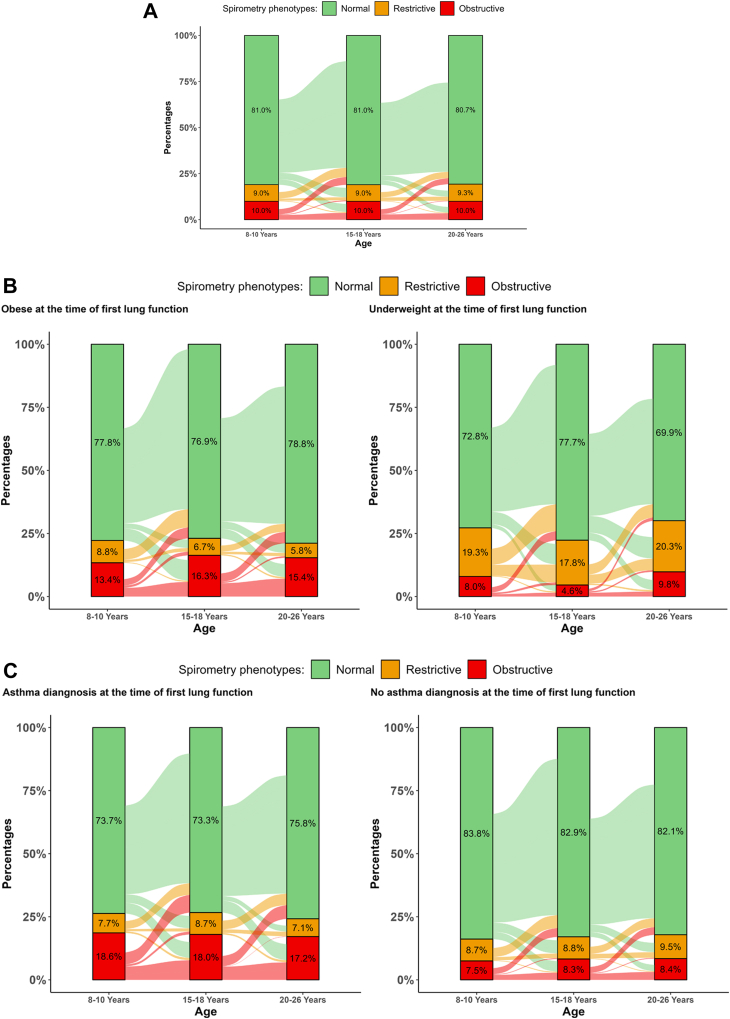
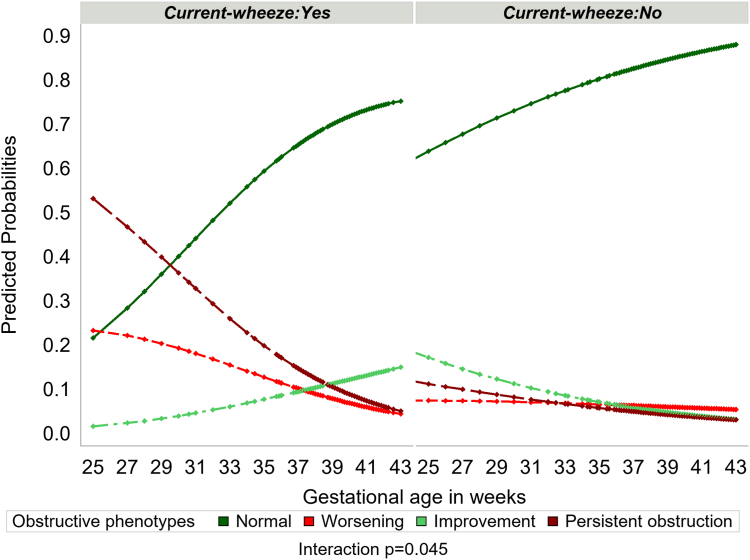
Obstructive phenotype was observed in ∼10%, and restrictive in ∼9%. A substantial proportion of children with impaired lung function in school age (between one third in obstructive and a half in restricted phenotype) improved and achieved normal and stable lung function to early adulthood. Of those with normal lung function in school-age, <5% declined to adulthood. Underweight restrictive and obese obstructive participants were less likely to transit to normal. Maternal smoking during pregnancy and current asthma diagnosis increased the risk of persistent obstruction and worsening. Significant associate of worsening in restrictive phenotypes was lower BMI at the first lung function assessment. Data-driven methodologies identified similar risk factors for obstructive and restrictive clusters.
The worsening and improvement in obstructive and restrictive spirometry were observed at all ages. Maintaining optimal weight during childhood and reducing maternal smoking during pregnancy may reduce spirometry obstruction and restriction and improve lung function.
MRC Grant MR/S025340/1.
肺量计检测出的阻塞性和限制性肺功能损害模式可预测健康状况不佳。我们研究了这些表型在儿童期至成年早期的发展及其转变情况。
在本研究中,我们分析了1989年至1995年间建立的三个英国人群出生队列的汇总数据。我们对来自三个基于人群的出生队列的数据应用了描述性统计、回归建模和数据驱动建模,这些队列从儿童期到成年期至少有三次肺功能检测(中学中期:8 - 10岁,n = 8404;青春期:15 - 18岁,n = 5764;成年早期:20 - 26岁,n = 4680)。根据调整后的回归残差将参与者分为正常、限制性和阻塞性肺量计检测组。我们考虑了两个转变阶段:从8 - 10岁到15 - 18岁以及从15 - 18岁到20 - 26岁。
观察到阻塞性表型的比例约为10%,限制性表型约为9%。学龄期肺功能受损的儿童中,相当一部分(阻塞性表型中有三分之一,限制性表型中有一半)情况有所改善,并在成年早期达到正常且稳定的肺功能。学龄期肺功能正常的儿童中,不到5%的人成年后肺功能下降。体重过轻的限制性和肥胖的阻塞性参与者转变为正常的可能性较小。孕期母亲吸烟和当前哮喘诊断增加了持续阻塞和病情恶化的风险。限制性表型病情恶化的一个重要相关因素是首次肺功能评估时较低的体重指数。数据驱动方法确定了阻塞性和限制性聚类的类似风险因素。
在所有年龄段均观察到阻塞性和限制性肺量计检测结果的恶化和改善情况。儿童期保持最佳体重以及孕期减少母亲吸烟可能会减少肺量计检测的阻塞和限制情况,并改善肺功能。
医学研究理事会资助项目MR/S025340/1。