Metheny Leland L, Sobecks Ronald, Cho Christina, Fu Pingfu, Margevicius Seunghee, Wang Jiasheng, Ciarrone Lisa, Kopp Shelby, Convents Robin D, Majhail Navneet, Caimi Paolo F, Otegbeye Folashade, Cooper Brenda W, Gallogly Molly, Malek Ehsan, Tomlinson Benjamin, Gerds Aaron T, Hamilton Betty, Giralt Sergio, Perales Miguel-Angel, de Lima Marcos
Hematology and Cell Therapy Division, Seidman Cancer Center, University Hospitals, Cleveland, OH.
Case Comprehensive Cancer Center, Cleveland, OH.
Blood Adv. 2024 Mar 26;8(6):1384-1391. doi: 10.1182/bloodadvances.2023011514.
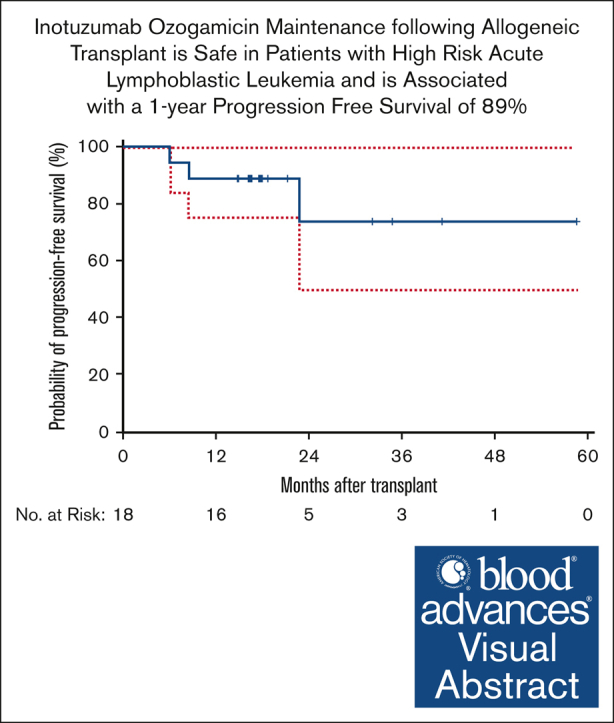
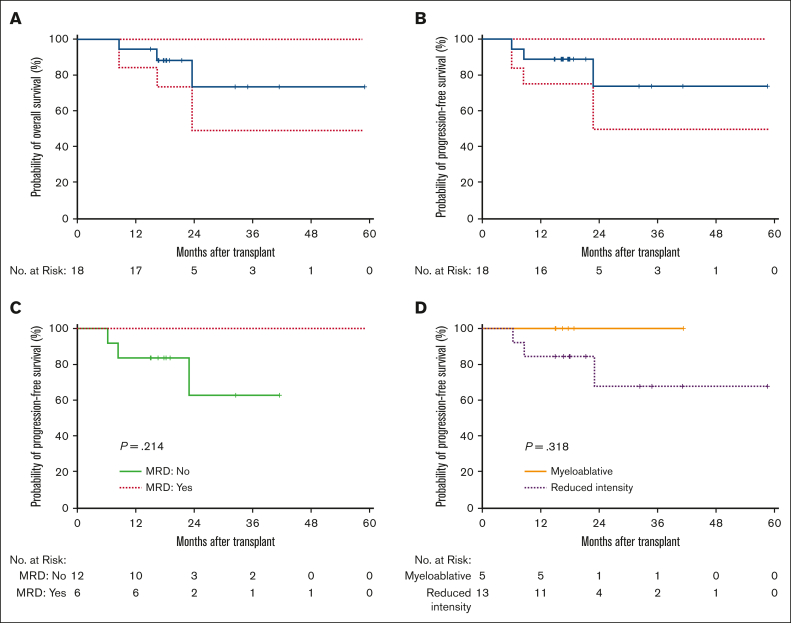
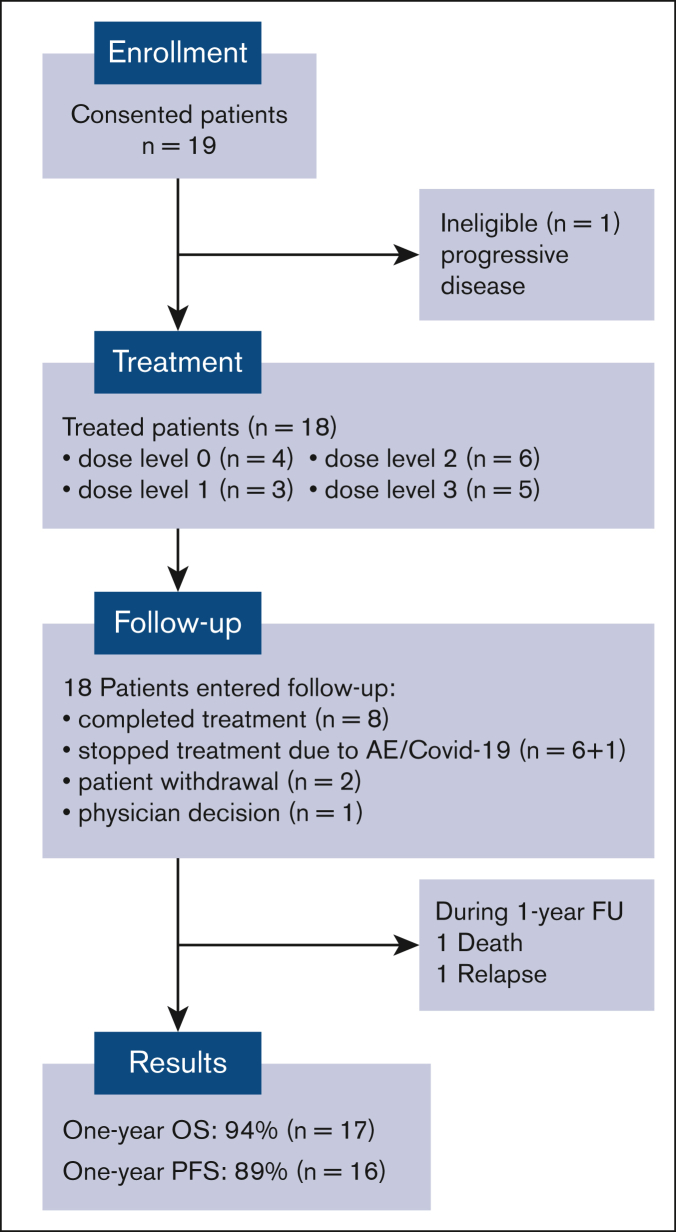
The curative potential of allogeneic hematopoietic transplantation (allo-HCT) in patients with acute lymphoblastic leukemia (ALL) is hampered by relapse. Inotuzumab ozogamicin (INO) is an anti-CD22 monoclonal antibody bound to calicheamicin, which has significant activity against ALL. We hypothesized that low-dose INO would be safe and feasible after allo-HCT. Therefore, we conducted a phase 1 study to determine the dose and safety in this setting. Patients were eligible if they were aged 16 to 75 years, had undergone allo-HCT for CD22+ ALL, were in complete remission (CR) after allo-HCT, had high risk of recurrence, were between day 40 and 100 after allo-HCT with adequate graft function, and did not have a history of sinusoidal obstruction syndrome (SOS). The objectives of this trial were to define INO maximum tolerated dose (MTD), to determine post-allo-HCT INO safety, and to measure 1-year progression-free survival (PFS). The trial design followed a "3+3" model. The treatment consisted of INO given on day 1 of 28-day cycles. Dose levels were 0.3 mg/m2, 0.4 mg/m2, 0.5 mg/m2, and 0.6 mg/m2. Median age was 44 years (range, 17-66 years; n = 18). Disease status at transplantation was first CR (n = 14) or second CR or beyond (n = 4). Preparative regimen was of reduced intensity in 72% of patients who received transplantation. Most common toxicity was thrombocytopenia. There were no instances of SOS; the MTD was 0.6 mg/m2. One-year nonrelapse mortality was 5.6%. With a median follow-up of 18.1 months (range, 8.6-59 months) 1-year post-allo-HCT PFS and overall survival is 89% and 94%, respectively. Low-dose INO has a favorable safety profile and was associated with high rates of 1-year PFS. This trial was registered at www.clinicaltrials.gov as #NCT03104491.
急性淋巴细胞白血病(ALL)患者接受异基因造血移植(allo-HCT)后的治愈潜力受到复发的阻碍。伊诺妥昔单抗(INO)是一种与卡奇霉素结合的抗CD22单克隆抗体,对ALL具有显著活性。我们假设低剂量INO在allo-HCT后是安全可行的。因此,我们开展了一项1期研究来确定这种情况下的剂量和安全性。年龄在16至75岁、因CD22+ ALL接受allo-HCT、allo-HCT后处于完全缓解(CR)状态、复发风险高、allo-HCT后40至100天且移植物功能良好且无肝窦阻塞综合征(SOS)病史的患者符合入选条件。本试验的目的是确定INO的最大耐受剂量(MTD)、确定allo-HCT后INO的安全性以及测量1年无进展生存期(PFS)。试验设计采用“3+3”模型。治疗包括在28天周期的第1天给予INO。剂量水平分别为0.3mg/m²、0.4mg/m²、0.5mg/m²和0.6mg/m²。中位年龄为44岁(范围1,7-66岁;n = 18)。移植时的疾病状态为首次CR(n = 14)或第二次CR及以上(n = 4)。72%接受移植的患者预处理方案为减低强度。最常见的毒性是血小板减少。未发生SOS病例;MTD为0.6mg/m²。1年非复发死亡率为5.6%。allo-HCT后1年,中位随访18.1个月(范围8.6-59个月),PFS和总生存率分别为89%和94%。低剂量INO具有良好的安全性,且与1年PFS的高发生率相关。本试验已在www.clinicaltrials.gov注册,注册号为#NCT03104491。