Dave Priya, Patel Rutul D, Desai Kush, Davila Jonathan, Sankin Alex
Department of Urology, Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, NY, USA.
Smith Institute for Urology, Northwell Health, Lake Success, NY, USA.
Bladder Cancer. 2023 Dec 13;9(4):335-344. doi: 10.3233/BLC-230074. eCollection 2023.
A lack of standardization is pervasive in procedural application and reporting templates for TURBT with the use of a surgical checklist proposed as a means for quality improvement.
To introduce a TURBT checklist to assess surgeon prediction accuracy and the impact of standardized documentation on quality of resection and oncologic outcomes.
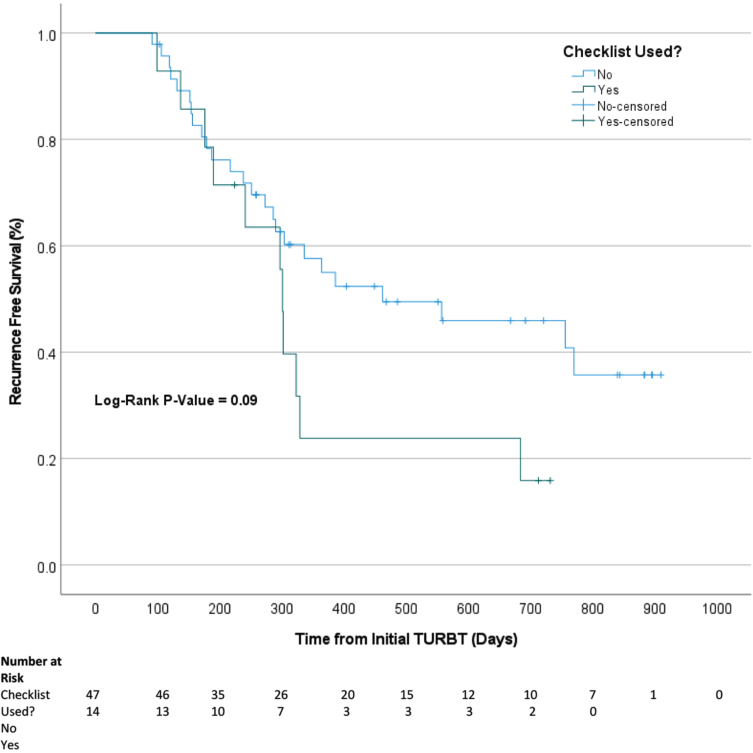
Nine critical elements of a high-quality TURBT identified by literature review were incorporated into a prospectively implemented checklist for operative reports. The checklist included both visualized and predicted tumor characteristics. A retrospective single-institution analysis compared quality of dictation pre- and post-checklist implementation. Surgeon predictions were compared to final pathology reports to determine rates of concordance. Kaplan-Meier curves examined the association of checklist use with recurrence free survival (RFS).
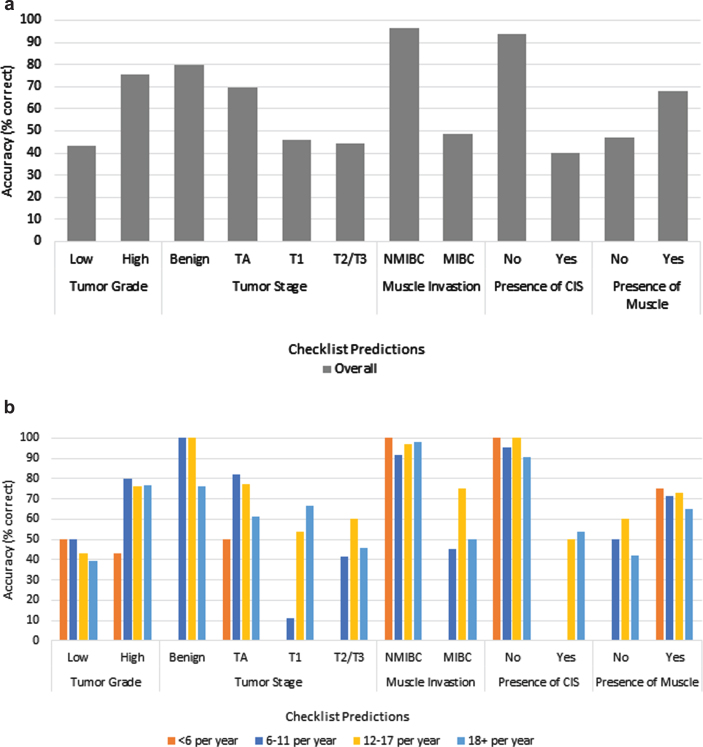
333 operative reports were included in this analysis, of which 107 (32.1%) were completed pre-checklist implementation. The average number of critical elements reported was 8.69 with checklist use compared to 4.99 without ( < 0.001). There was no significant difference in RFS between the pre- and post-checklist cohorts (log-rank test = 0.53). Surgeons were least and most accurate in predicting low grade tumor (43.5%) and absence of muscle invasion (96.6%), respectively.
Incorporation of a TURBT surgical checklist improves operative dictation and quality of reporting but did not directly impact RFS. With quality of initial resection a proven correlate to recurrence rates, checklist implementation to improve surgical performance and long-term oncologic outcomes reveals an interesting area of exploration highlighting the need for more standardized methodology when performing these procedures.
经尿道膀胱肿瘤切除术(TURBT)的程序应用和报告模板普遍缺乏标准化,有人提出使用手术检查表作为提高质量的一种手段。
引入一份TURBT检查表,以评估外科医生的预测准确性以及标准化文档对切除质量和肿瘤学结果的影响。
通过文献综述确定的高质量TURBT的九个关键要素被纳入前瞻性实施的手术报告检查表中。该检查表包括可视化和预测的肿瘤特征。一项回顾性单机构分析比较了检查表实施前后的口述质量。将外科医生的预测与最终病理报告进行比较,以确定一致性率。Kaplan-Meier曲线检验了检查表使用与无复发生存率(RFS)之间的关联。
本分析纳入了333份手术报告,其中107份(32.1%)是在检查表实施前完成的。使用检查表时报告的关键要素平均数量为8.69个,而不使用检查表时为4.99个(<0.001)。检查表实施前后的RFS队列之间没有显著差异(对数秩检验=0.53)。外科医生在预测低级别肿瘤(43.5%)和无肌肉浸润(96.6%)方面的准确性最低和最高。
纳入TURBT手术检查表可改善手术口述和报告质量,但并未直接影响RFS。由于初始切除质量已被证明与复发率相关,实施检查表以提高手术性能和长期肿瘤学结果揭示了一个有趣的探索领域,突出了在进行这些手术时需要更标准化方法的必要性。