Department of Global Public Health, Karolinska Institutet, Stockholm, Sweden.
Department of Statistics, Center for Research in Human Reproduction and Demography, Cotonou, Benin.
Acta Obstet Gynecol Scand. 2024 Mar;103(3):590-601. doi: 10.1111/aogs.14754. Epub 2024 Jan 6.
Birth asphyxia is a leading cause of neonatal mortality in sub-Saharan Africa. The relationship to grand multiparity (GM), a controversial pregnancy risk factor, remains largely unexplored, especially in the context of large multinational studies. We investigated birth asphyxia and its association with GM and referral in Benin, Malawi, Tanzania and Uganda.
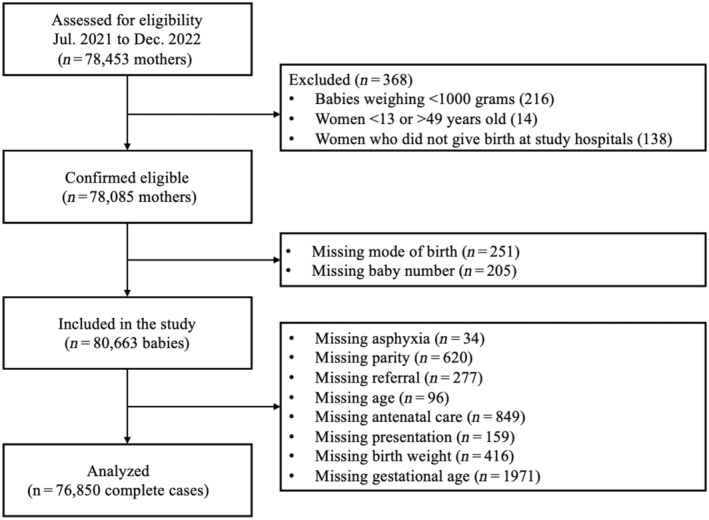
This was a prospective cross-sectional study. Data were collected using a perinatal e-Registry in 16 hospitals (four per country). The study population consisted of 80 663 babies (>1000 g, >28 weeks' gestational age) delivered between July 2021 and December 2022. The primary outcome was birth asphyxia, defined by 5-minute appearance, pulse, grimace, activity and respiration score <7. A multilevel and stratified multivariate logistic regression was performed with GM (parity ≥5) as exposure, and birth asphyxia as outcome. An interaction between referral (none, prepartum, intrapartum) and GM was also evaluated as a secondary outcome. All models were adjusted for confounders.
Pan African Clinical Trial Registry 202006793783148.
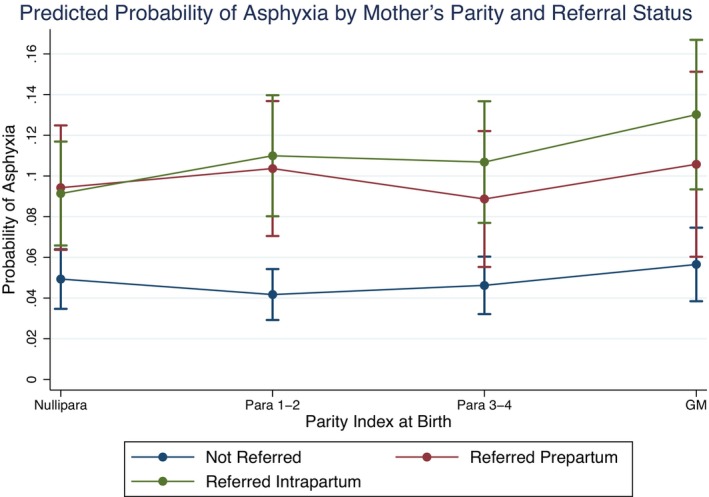
Birth asphyxia was present in 7.0% (n = 5612) of babies. More babies with birth asphyxia were born to grand multiparous women (11.9%) than to other parity groups (≤7.6%). Among the 76 850 cases included in the analysis, grand multiparous women had a 1.34 times higher odds of birth asphyxia (95% confidence interval [CI] 1.17-1.54) vs para one to two. Grand multiparous women referred intrapartum had the highest probability of asphyxiation (13.02%, 95% CI 9.34-16.69). GM increased odds of birth asphyxia in Benin (odds ratio [OR] 1.37, 95% CI 1.13-1.68) and Uganda (OR 1.29, 95% CI 1.02-1.64), but was non-significant in Tanzania (OR 1.44, 95% CI 0.81-2.56) and Malawi (OR 0.98, 95% CI 0.67-1.44).
There is some evidence of an increased risk of birth asphyxia for grand multiparous women having babies at hospitals, especially following intrapartum referral. Antenatal counseling should recognize grand multiparity as higher risk and advise appropriate childbirth facilities. Findings in Malawi suggest an advantage of health systems configuration requiring further exploration.
在撒哈拉以南非洲,出生窒息是新生儿死亡的主要原因。与备受争议的妊娠风险因素——多胎妊娠(GM)的关系在很大程度上仍未得到探索,特别是在大型跨国研究中。我们在贝宁、马拉维、坦桑尼亚和乌干达调查了出生窒息及其与 GM 和转诊的关系。
这是一项前瞻性的横断面研究。数据通过 16 家医院(每个国家 4 家)的围产期电子登记处收集。研究人群由 2021 年 7 月至 2022 年 12 月期间分娩的体重超过 1000 克(≥28 周)的 80663 名婴儿组成。主要结局为出生窒息,定义为 5 分钟时的外观、脉搏、面部表情、活动和呼吸评分<7。使用 GM(产次≥5)作为暴露因素,出生窒息作为结局,进行多水平和分层多变量逻辑回归。还评估了转诊(无、产前、产时)和 GM 之间的相互作用作为次要结局。所有模型均针对混杂因素进行了调整。
泛非临床试验注册处 202006793783148。
出生窒息发生在 7.0%(n=5612)的婴儿中。出生窒息的婴儿中 GM 产妇(11.9%)比其他产次组(≤7.6%)的婴儿更多。在纳入分析的 76850 例病例中,GM 产妇发生出生窒息的几率是产次为 1-2 次的产妇的 1.34 倍(95%置信区间[CI] 1.17-1.54)。GM 产妇产时转诊的窒息概率最高(13.02%,95% CI 9.34-16.69)。GM 增加了贝宁(比值比[OR] 1.37,95% CI 1.13-1.68)和乌干达(OR 1.29,95% CI 1.02-1.64)出生窒息的几率,但在坦桑尼亚(OR 1.44,95% CI 0.81-2.56)和马拉维(OR 0.98,95% CI 0.67-1.44)中无统计学意义。
有一些证据表明,GM 产妇在医院分娩的婴儿出生窒息的风险增加,尤其是在产时转诊后。产前咨询应认识到 GM 是更高的风险,并建议适当的分娩设施。在马拉维的研究结果表明,卫生系统配置的优势需要进一步探索。