Gołąbek Natalia, Jakubowski Wojciech, Król Szymon, Kozioł Mateusz, Niewiara Łukasz, Kleczyński Paweł, Legutko Jacek, Dziewierz Artur, Surdacki Andrzej, Chyrchel Michał
Students' Scientific Group at the Second Department of Cardiology, Jagiellonian University Medical College, Krakow, Poland.
Students' Scientific Group of Modern Cardiac Therapy at the Department of Interventional Cardiology, Jagiellonian University Medical College, John Paul II Hospital, Krakow, Poland.
Postepy Kardiol Interwencyjnej. 2023 Dec;19(4):326-332. doi: 10.5114/aic.2023.132161. Epub 2023 Oct 18.
Electrocardiographic (ECG) patterns suggestive of high-risk coronary anatomy are indications for an urgent invasive approach in non-ST-segment elevation acute coronary syndrome (NSTE-ACS).
To estimate the frequency of the observed phenomenon and assess the clinical characteristics of NSTE-ACS subjects associated with Wellens syndrome, the de Winter sign, or ST-segment depressions by ≥ 1 mm in ≥ 6 classic ECG leads with simultaneous ST-segment elevation in aVR and/or V1.
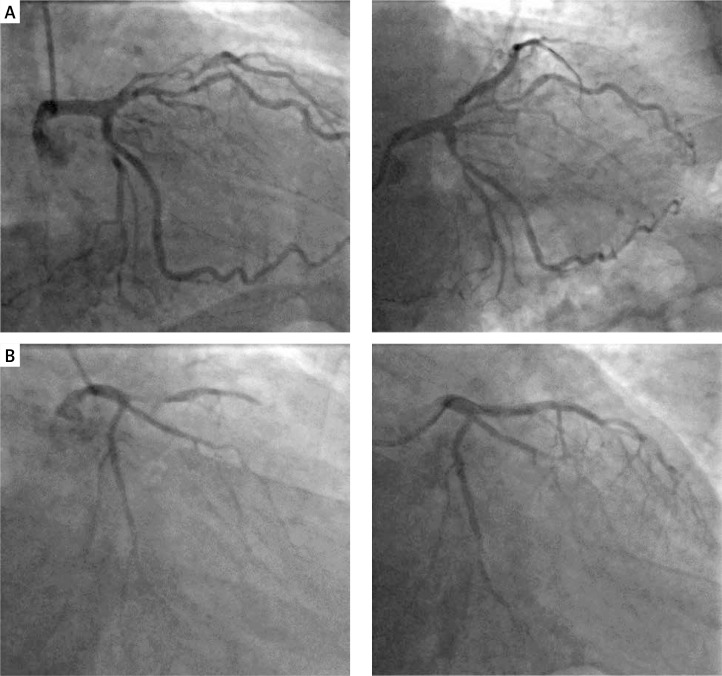
Out of 207 pre-screened subjects diagnosed with NSTE-ACS, 64 patients (26 women and 38 men) with complete medical records (including admission ECG and coronary angiography during the index hospitalization), and significant culprit stenosis or occlusion of the left main coronary artery (LMCA) or the proximal/middle segment of the left anterior descending artery (LAD) entered the final analysis. Clinical characteristics of patients exhibiting any of the high-risk ECG patterns was compared to their counterparts with significant lesions in LMCA or proximal/middle LAD without any of the high-risk ECG patterns.
Among 64 patients with significant culprit lesions in LMCA or LAD, 19 (29.69%) exhibited one of the high-risk ECG patterns: Wellens syndrome ( = 10), the de Winter sign ( = 0), or multiple ST-segment depressions ( = 9). Clinical characteristics were comparable in 19 NSTE-ACS patients with the high-risk ECG patterns and their 45 counterparts.
Because ECG patterns suggestive of high-risk coronary anatomy are relatively frequent in patients with NSTE-ACS and culprit lesions in LMCA or LAD, their early recognition is of clinical importance.
提示高危冠状动脉解剖结构的心电图(ECG)模式是非ST段抬高型急性冠状动脉综合征(NSTE-ACS)紧急侵入性治疗方法的指征。
评估观察到的现象的发生率,并评估与Wellens综合征、de Winter征或≥6个经典ECG导联中ST段压低≥1mm且同时aVR和/或V1导联ST段抬高相关的NSTE-ACS患者的临床特征。
在207名经预筛查诊断为NSTE-ACS的患者中,64例患者(26名女性和38名男性)有完整的病历记录(包括入院时的ECG和本次住院期间的冠状动脉造影),且左主干冠状动脉(LMCA)或左前降支动脉(LAD)近端/中段存在明显的罪犯病变狭窄或闭塞,纳入最终分析。将表现出任何一种高危ECG模式的患者的临床特征与其LMCA或LAD近端/中段有明显病变但无任何高危ECG模式的患者进行比较。
在64例LMCA或LAD有明显罪犯病变的患者中,19例(29.69%)表现出一种高危ECG模式:Wellens综合征(=十)、de Winter征(=0)或多个ST段压低(=9)。19例有高危ECG模式的NSTE-ACS患者与其45例对照者的临床特征具有可比性。
由于提示高危冠状动脉解剖结构的ECG模式在NSTE-ACS患者以及LMCA或LAD有罪犯病变的患者中相对常见,因此早期识别具有临床重要性。