Division of General Internal Medicine, Department of Medicine, Cedars-Sinai Medical Center, Los Angeles, California.
Department of Health Policy and Management, Fielding School of Public Health, University of California, Los Angeles.
JAMA Netw Open. 2024 Jan 2;7(1):e2350963. doi: 10.1001/jamanetworkopen.2023.50963.
Polypharmacy is associated with mortality, falls, hospitalizations, and functional and cognitive decline. The study of polypharmacy-related interventions has increased substantially, prompting the need for an updated, more focused systematic overview.
To systematically evaluate and summarize evidence across multiple systematic reviews (SRs) examining interventions addressing polypharmacy.
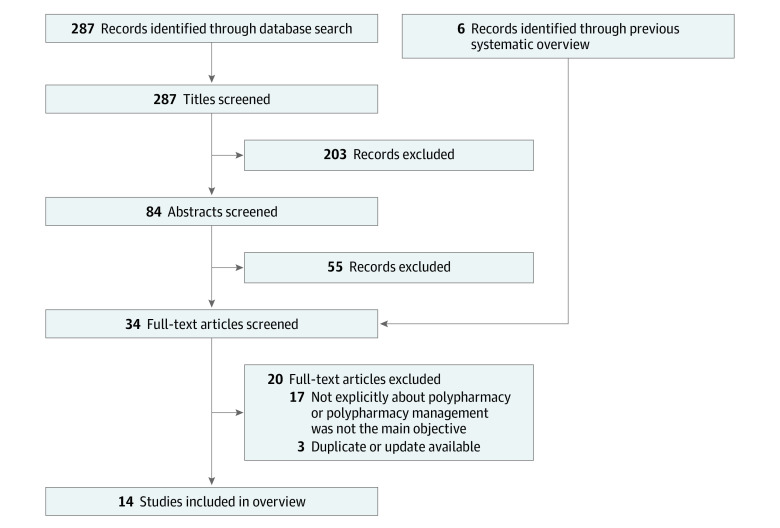
A search was conducted of MEDLINE, the Cochrane Database of Systematic Reviews, and the Database of Abstracts of Reviews of Effects for articles published from January 2017-October 2022, as well as those identified in a previous overview (January 2004-February 2017). Systematic reviews were included regardless of study design, setting, or outcome. The evidence was summarized by 4 categories: (1) medication-related process outcomes (eg, potentially inappropriate medication [PIM] and potential prescribing omission reductions), (2) clinical and functional outcomes, (3) health care use and economic outcomes, and (4) acceptability of the intervention.
Fourteen SRs were identified (3 from the previous overview), 7 of which included meta-analyses, representing 179 unique published studies. Nine SRs examined medication-related process outcomes (low to very low evidence quality). Systematic reviews using pooled analyses found significant reductions in the number of PIMs, potential prescribing omissions, and total number of medications, and improvements in medication appropriateness. Twelve SRs examined clinical and functional outcomes (very low to moderate evidence quality). Five SRs examined mortality; all mortality meta-analyses were null, but studies with longer follow-up periods found greater reductions in mortality. Five SRs examined falls incidence; results were predominantly null save for a meta-analysis in which PIMs were discontinued. Of the 8 SRs examining quality of life, most (7) found predominantly null effects. Ten SRs examined hospitalizations and readmissions (very low to moderate evidence quality) and 4 examined emergency department visits (very low to low evidence quality). One SR found significant reductions in hospitalizations and readmissions among higher-intensity medication reviews with face-to-face patient components. Another meta-analysis found a null effect. Of the 7 SRs without meta-analyses for hospitalizations and readmissions, all had predominantly null results. Two of 4 SRs found reductions in emergency department visits. Two SRs examined acceptability (very low evidence quality), finding wide variation in the adoption of polypharmacy-related interventions.
This updated systematic overview noted little evidence of an association between polypharmacy-related interventions and reduced important clinical and health care use outcomes. More evidence is needed regarding which interventions are most useful and which populations would benefit most.
药物过多与死亡率、跌倒、住院、功能和认知能力下降有关。针对药物过多相关干预措施的研究大幅增加,这促使我们需要更新更集中的系统综述。
系统评估和总结多项系统评价(SRs)中审查干预药物过多的证据。
对 MEDLINE、Cochrane 系统评价数据库和效应摘要数据库进行了搜索,检索范围为 2017 年 1 月至 2022 年 10 月发表的文章,以及之前综述(2004 年 1 月至 2017 年 2 月)中确定的文章。无论研究设计、设置或结果如何,都纳入了系统评价。证据按 4 个类别进行总结:(1)药物相关过程结果(如潜在不适当药物 [PIM] 和潜在处方遗漏减少),(2)临床和功能结果,(3)医疗保健使用和经济结果,(4)干预措施的可接受性。
确定了 14 项 SR(其中 3 项来自之前的综述),其中 7 项包含荟萃分析,代表了 179 项已发表的独特研究。9 项 SR 研究了药物相关过程结果(低至非常低的证据质量)。使用汇总分析的系统评价发现,PIM、潜在处方遗漏和药物总数显著减少,药物适当性得到改善。12 项 SR 研究了临床和功能结果(非常低至中等证据质量)。5 项 SR 研究了死亡率;所有死亡率荟萃分析均为无效,但随访时间较长的研究发现死亡率降低幅度更大。5 项 SR 研究了跌倒发生率;结果主要为无效,除了一项 PIM 被停用的荟萃分析外。在 8 项研究生活质量的 SR 中,大多数(7 项)发现主要为无效影响。10 项 SR 研究了住院和再入院(低至中等证据质量)和 4 项研究了急诊就诊(低至低证据质量)。一项 SR 发现,面对面患者组成的更高强度药物审查可显著减少住院和再入院。另一项荟萃分析发现无效。对于没有住院和再入院荟萃分析的 7 项 SR,所有结果均主要为无效。4 项 SR 中有 2 项发现急诊就诊次数减少。两项 SR 研究了可接受性(非常低的证据质量),发现与药物过多相关的干预措施的采用差异很大。
本更新的系统综述注意到,药物过多相关干预措施与减少重要临床和医疗使用结果之间几乎没有关联的证据。需要更多证据来确定哪些干预措施最有用,哪些人群受益最大。