Janczak Joanna, Ukegjini Kristjan, Bischofberger Stephan, Turina Matthias, Müller Philip C, Steffen Thomas
Clinic for General and Visceral Surgery, Hospital for the Region Fürstenland Toggenburg, CH-9500 Wil, Switzerland.
Department of Surgery, Hospital of the Canton of St. Gallen, CH-9007 St. Gallen, Switzerland.
Cancers (Basel). 2023 Dec 20;16(1):26. doi: 10.3390/cancers16010026.
Randomised controlled trials (RCTs) continue to provide the best evidence for treatment options, but the quality of reporting in RCTs and the completeness rate of reporting of surgical outcomes and complication data vary widely. The aim of this study was to measure the quality of reporting of the surgical outcome and complication data in RCTs of rectal cancer treatment and whether this quality has changed over time.
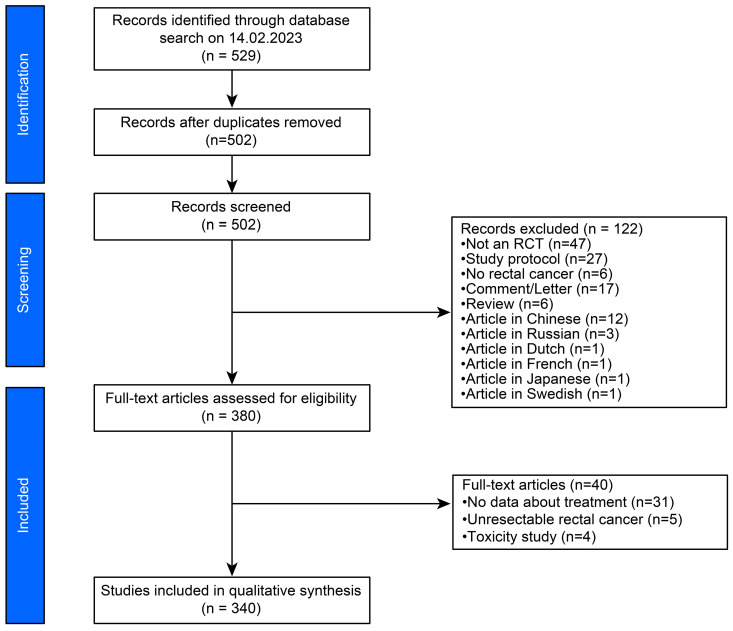
Eligible articles with the keywords ("rectal cancer" OR "rectal carcinoma") AND ("radiation" OR "radiotherapy") that were RCTs and published in the English, German, Polish, or Italian language were identified by reviewing all abstracts published from 1982 through 2022. Two authors independently screened and analysed all studies. The quality of the surgical outcome and complication data was assessed based on fourteen criteria, and the quality of RCTs was evaluated based on a modified Jadad scale. The primary outcome was the quality of reporting in RCTs and the completeness rate of reporting of surgical results and complication data.
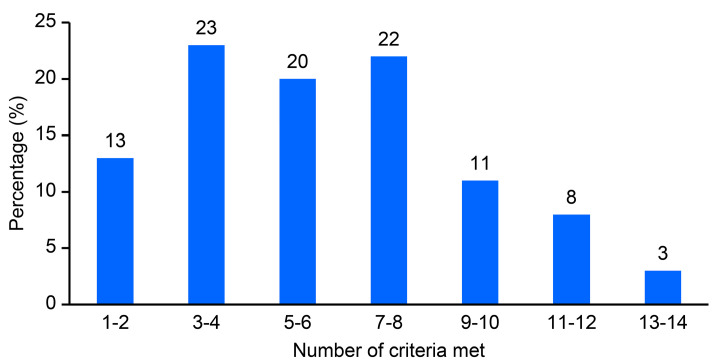
A total of 340 articles reporting multimodal therapy outcomes for 143,576 rectal cancer patients were analysed. A total of 7 articles (2%) met all 14 reporting criteria, 13 met 13 criteria, 27 met from 11 to 12 criteria, 36 met from 9 to 10 criteria, 76 met from 7 to 8 criteria, and most articles met fewer than 7 criteria (mean 5.5 criteria). Commonly underreported criteria included complication severity (15% of articles), macroscopic integrity of mesorectal excision (17% of articles), length of stay (18% of articles), number of lymph nodes (21% of articles), distance between the tumour and circumferential resection margin (CRM) (26% of articles), surgical radicality according to the site of the primary tumour (R0 vs. R1 + R2) (29% of articles), and CRM status (38% of articles).
Inconsistent surgical outcome and complication data reporting in multimodal rectal cancer treatment RCTs is standard. Standardised reporting of clinical and oncological outcomes should be established to facilitate comparing studies and results of related research topics.
随机对照试验(RCT)仍然是治疗方案最佳证据的来源,但RCT报告的质量以及手术结果和并发症数据的报告完整率差异很大。本研究的目的是衡量直肠癌治疗RCT中手术结果和并发症数据的报告质量,以及该质量是否随时间变化。
通过检索1982年至2022年发表的所有摘要,确定符合条件的文章,关键词为(“直肠癌”或“直肠癌”)以及(“放射”或“放射治疗”),且为RCT,发表语言为英语、德语、波兰语或意大利语。两位作者独立筛选和分析所有研究。根据14项标准评估手术结果和并发症数据的质量,并根据改良的Jadad量表评估RCT的质量。主要结果是RCT报告的质量以及手术结果和并发症数据的报告完整率。
共分析了340篇报告143,576例直肠癌患者多模式治疗结果的文章。共有7篇文章(2%)符合所有14项报告标准,13篇符合13项标准,27篇符合11至12项标准,36篇符合9至10项标准,76篇符合7至8项标准,大多数文章符合少于7项标准(平均5.5项标准)。常见的报告不足标准包括并发症严重程度(15%的文章)、直肠系膜切除的宏观完整性(17%的文章)、住院时间(18%的文章)、淋巴结数量(21%的文章)、肿瘤与环周切缘(CRM)的距离(26%的文章)、根据原发肿瘤部位的手术根治性(R0与R1+R2)(29%的文章)以及CRM状态(38%的文章)。
多模式直肠癌治疗RCT中手术结果和并发症数据报告不一致是常态。应建立临床和肿瘤学结果的标准化报告,以促进相关研究主题的研究和结果比较。