Upadhyay Rituraj, Klamer Brett G, Perlow Haley K, White Julia R, Bazan Jose G, Jhawar Sachin R, Blakaj Dukagjin M, Grecula John C, Arnett Andrea, Mestres-Villanueva Mariella A, Healy Erin H, Thomas Evan M, Chakravarti Arnab, Raval Raju R, Lustberg Maryam, Williams Nicole O, Palmer Joshua D, Beyer Sasha J
Department of Radiation Oncology, The Ohio State University Comprehensive Cancer Center, Columbus, OH 43210, USA.
Department of Biostatistics, The Ohio State University Comprehensive Cancer Center, Columbus, OH 43210, USA.
Cancers (Basel). 2023 Dec 27;16(1):137. doi: 10.3390/cancers16010137.
Breast cancer is the second most common cause of brain metastases (BM). Despite increasing incidence of BM in older women, there are limited data on the optimal management of BM in this age group. In this study, we assessed the survival outcomes and treatment patterns of older breast cancer patients ≥65 years old with BM compared to younger patients at our institution.
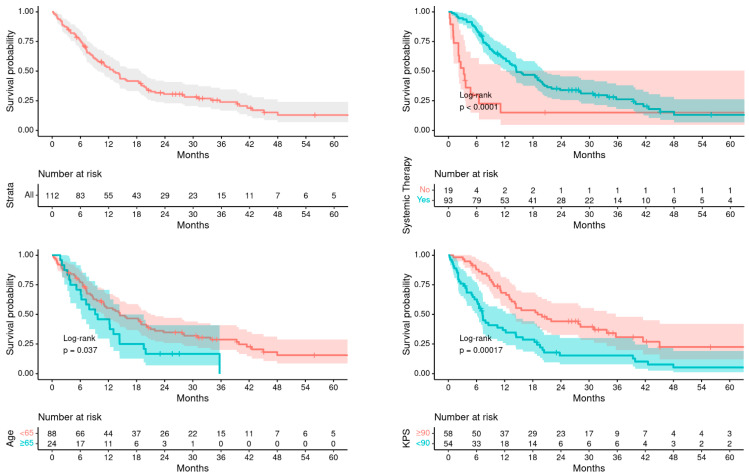
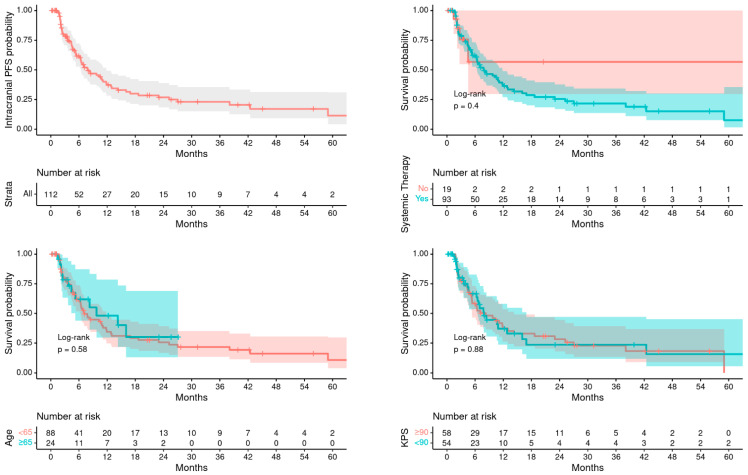
An IRB-approved single-institutional retrospective review of biopsy-proven breast cancer patients with BM treated with 1- to 5-fraction stereotactic radiation therapy (SRS) from 2015 to 2020 was performed. Primary endpoint was intracranial progression-free survival (PFS) defined as the time interval between the end of SRS to the date of the first CNS progression. Secondary endpoints were overall survival (OS) from the end of SRS and radiation treatment patterns. Kaplan-Meier estimates and Cox proportional hazard regression method were used for survival analyses.
A total of 112 metastatic breast cancer patients with BMs were included of which 24 were ≥65 years old and 88 were <65 years old. Median age at RT was 72 years (range 65-84) compared to 52 years (31-64) in younger patients. There were significantly higher number of older women with ER/PR positive disease (75% vs. 49%, = 0.036), while younger patients were more frequently triple negative (32% vs. 12%, = 0.074) and HER2 positive (42% vs. 29%, = 0.3). Treatment-related adverse events were similar in both groups. Overall, 14.3% patients had any grade radiation necrosis (RN) (older vs. young: 8.3% vs. 16%, = 0.5) while 5.4% had grade 3 or higher RN (0% vs. 6.8%, = 0.7). Median OS after RT was poorer in older patients compared to younger patients (9.5 months vs. 14.5 months, = 0.037), while intracranial PFS from RT was similar between the two groups (9.7 months vs. 7.1 months, = 0.580). On univariate analysis, significant predictors of OS were age ≥65 years old (hazard risk, HR = 1.70, = 0.048), KPS ≤ 80 (HR = 2.24, < 0.001), HER2 positive disease (HR = 0.46, < 0.001), isolated CNS metastatic disease (HR = 0.29, < 0.001), number of brain metastases treated with RT (HR = 1.06, = 0.028), and fractionated SRS (HR = 0.53, = 0.013). On multivariable analysis, KPS ≤ 80, HER2 negativity and higher number of brain metastases predicted for poorer survival, while age was not a significant factor for OS after adjusting for other variables. Patients who received systemic therapy after SRS had a significantly improved OS on univariate and multivariable analysis (HR = 0.32, < 0.001). Number of brain metastases treated was the only factor predictive of worse PFS (HR = 1.06, = 0.041), which implies a 6% additive risk of progression for every additional metastasis treated.
Although older women had poorer OS than younger women, OS was similar after adjusting for KPS, extracranial progression, and systemic therapy; and there was no difference in rates of intracranial PFS, neurological deaths, and LMD in the different age groups. This study suggests that age alone may not play an independent role in treatment-selection and that outcomes for breast cancer patients with BMs and personalized decision-making including other clinical factors should be considered. Future studies are warranted to assess neurocognitive outcomes and other radiation treatment toxicities in older patients.
乳腺癌是脑转移(BM)的第二大常见病因。尽管老年女性中BM的发病率不断上升,但关于该年龄组BM最佳治疗方法的数据有限。在本研究中,我们评估了我院65岁及以上老年乳腺癌BM患者与年轻患者的生存结局和治疗模式。
对2015年至2020年接受1至5次分割立体定向放射治疗(SRS)的经活检证实的乳腺癌BM患者进行了一项经机构审查委员会批准的单机构回顾性研究。主要终点是颅内无进展生存期(PFS),定义为SRS结束至首次中枢神经系统进展日期之间的时间间隔。次要终点是SRS结束后的总生存期(OS)和放射治疗模式。采用Kaplan-Meier估计法和Cox比例风险回归方法进行生存分析。
共纳入112例转移性乳腺癌BM患者,其中24例年龄≥65岁,88例年龄<65岁。放疗时的中位年龄为72岁(范围65-84岁),而年轻患者为52岁(31-64岁)。ER/PR阳性疾病的老年女性数量显著更多(75%对49%;P=0.036),而年轻患者更常为三阴性(32%对12%;P=0.074)和HER2阳性(42%对29%;P=0.3)。两组的治疗相关不良事件相似。总体而言,14.3%的患者发生了任何级别的放射性坏死(RN)(老年组对年轻组:8.3%对16%;P=0.5),而5.4%的患者发生了3级或更高级别的RN(0%对6.8%;P=0.7)。与年轻患者相比,老年患者放疗后的中位OS较差(9.5个月对14.5个月;P=0.037),而两组放疗后的颅内PFS相似(9.7个月对7.1个月;P=0.580)。单因素分析显示,OS的显著预测因素为年龄≥65岁(风险比,HR=1.70;P=0.048)、KPS≤80(HR=2.24;P<0.001)、HER2阳性疾病(HR=0.46;P<0.001)、孤立性中枢神经系统转移性疾病(HR=0.29;P<0.001)、接受放疗的脑转移灶数量(HR=1.06;P=0.028)和分割SRS(HR=0.53;P=0.013)。多因素分析显示,KPS≤80、HER2阴性和脑转移灶数量较多预示着生存较差,而在调整其他变量后,年龄不是OS的显著因素。在单因素和多因素分析中,SRS后接受全身治疗的患者OS显著改善(HR=0.32;P<0.001)。接受治疗的脑转移灶数量是唯一预测PFS较差的因素(HR=1.06;P=0.041),这意味着每多治疗一个转移灶,进展风险增加6%。
尽管老年女性的OS比年轻女性差,但在调整KPS、颅外进展和全身治疗后,OS相似;不同年龄组的颅内PFS、神经死亡和软脑膜转移率没有差异。本研究表明,仅年龄可能在治疗选择中不发挥独立作用,对于BM乳腺癌患者的结局和包括其他临床因素在内的个性化决策应予以考虑。未来有必要开展研究评估老年患者的神经认知结局和其他放射治疗毒性。