Chang Tou Pin, Ali Oroog, Tsimogiannis Kostas, Sica Giuseppe S, Khan Jim S
Epsom and St. Helier University Hospitals NHS Trust, Carshalton SM5 1AA, UK.
Gateshead Health NHS Foundation Trust, Gateshead NE9 6SX, UK.
J Clin Med. 2023 Dec 23;13(1):90. doi: 10.3390/jcm13010090.
The role of robotic lateral pelvic lymph node dissection (LPLND) for lateral pelvic nodal disease (LPND) in rectal cancer has yet to be investigated in the Western hemisphere. This study aims to investigate the safety and feasibility of robotic LPLND by utilising a well-established totally robotic TME protocol.
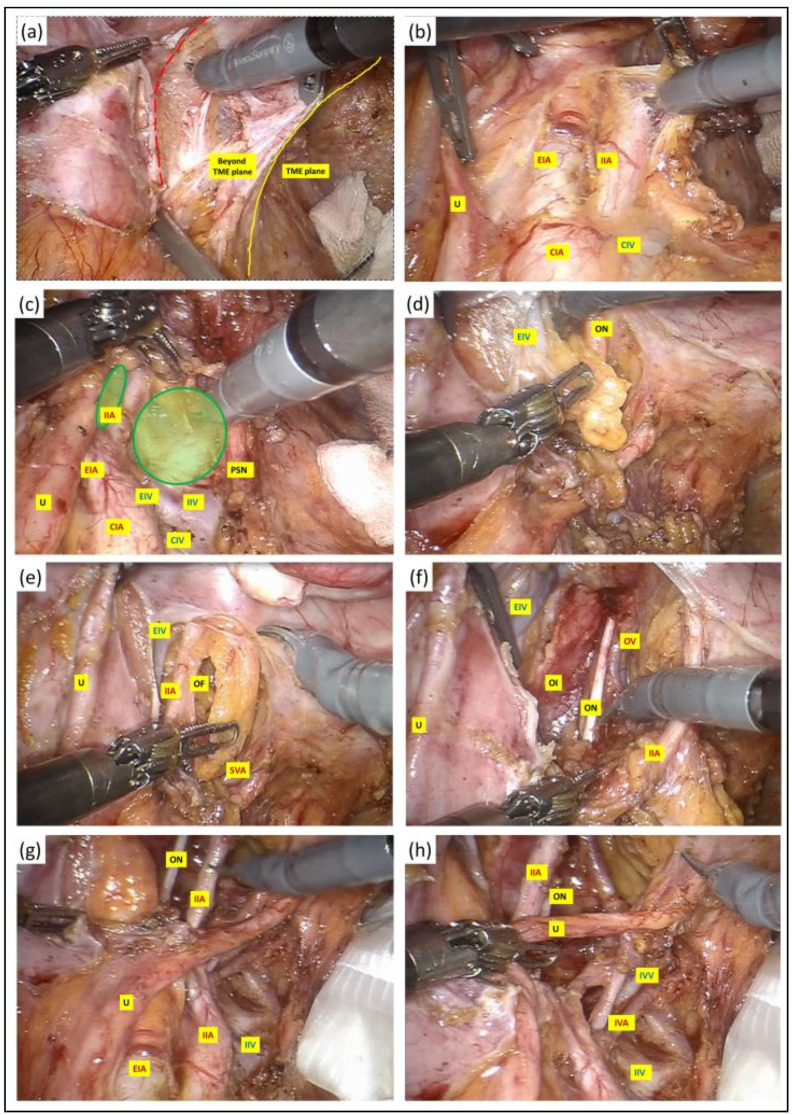
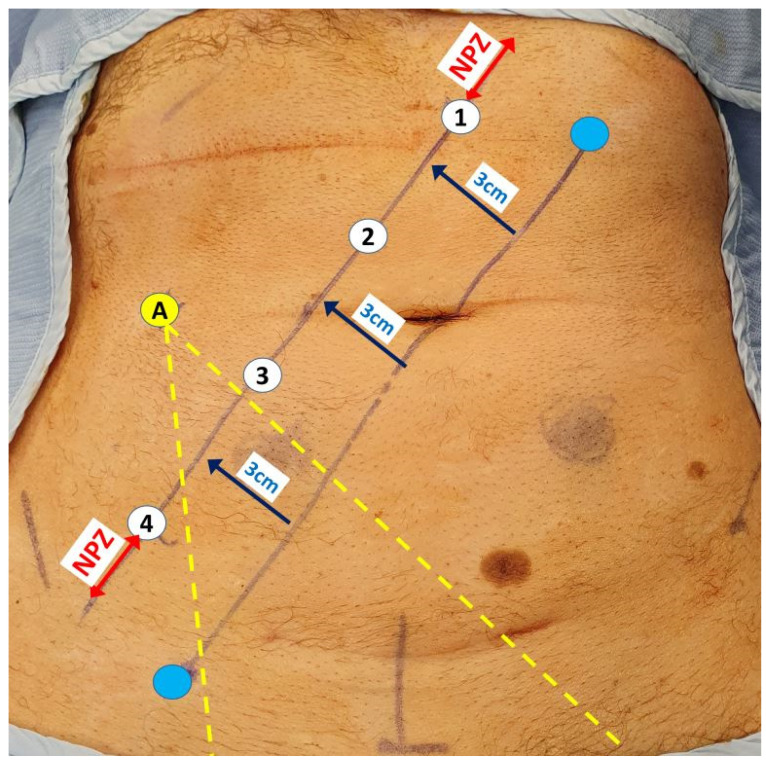
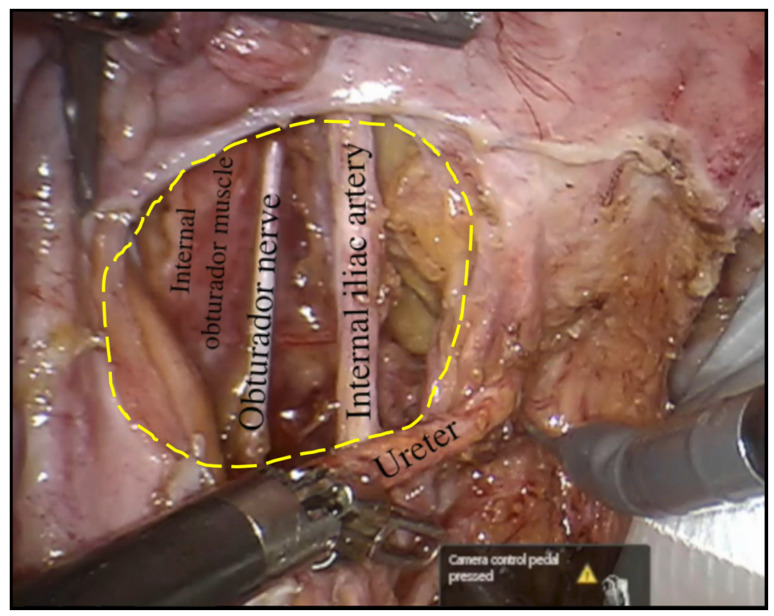
We conducted a retrospective study on 17 consecutive patients who underwent robotic LPLND for LPND ± TME for rectal cancer between 2015 and 2021. A single docking totally robotic approach from the left hip with full splenic mobilisation was performed using the X/Xi da Vinci platform. All patients underwent a tri-compartmental robotic en bloc excision of LPND with preservation of the obturator nerve and pelvic nerve plexus, leaving a well-skeletonised internal iliac vessel and its branches.
The median operative time was 280 min, which was 40 min longer than our standard robotic TME. The median BMI was 26, and there were no conversions. The median inpatient stay was 7 days with no Clavien-Dindo > 3 complications. One patient (6%) developed local recurrence and metastatic disease within 5 months. The proportion of histologically confirmed LPND was 41%, of which 94% were well to moderately differentiated adenocarcinoma. Median pre-operative lateral pelvic node size was significantly higher in positive nodes (14 mm vs. 8 mm ( = 0.01)). All patients had clear resection margins on histology.
Robotic LPLND is safe and feasible with good peri-operative and short-term outcomes, with the ergonomic advantages of a robotic TME docking protocol readily transferrable in LPLND.
在西半球,机器人辅助下的侧方盆腔淋巴结清扫术(LPLND)在直肠癌侧方盆腔淋巴结疾病(LPND)中的作用尚未得到研究。本研究旨在通过采用成熟的全机器人直肠癌根治术(TME)方案,探讨机器人辅助LPLND的安全性和可行性。
我们对2015年至2021年间连续17例因LPND±TME接受机器人辅助LPLND的直肠癌患者进行了回顾性研究。使用X/Xi达芬奇平台,从左髋部采用单对接全机器人方法,充分游离脾脏。所有患者均接受了LPND的三室机器人整块切除,保留闭孔神经和盆腔神经丛,使髂内血管及其分支呈现良好的骨骼化状态。
中位手术时间为280分钟,比我们的标准机器人TME长40分钟。中位体重指数(BMI)为26,无中转开腹病例。中位住院时间为7天,无Clavien-Dindo>3级并发症。1例患者(6%)在5个月内出现局部复发和转移性疾病。组织学确诊为LPND的比例为41%,其中94%为高分化至中分化腺癌。阳性淋巴结的术前侧方盆腔淋巴结中位大小显著更高(14毫米对8毫米(P=0.01))。所有患者组织学切缘均阴性。
机器人辅助LPLND是安全可行的,围手术期和短期效果良好,机器人TME对接方案的人体工程学优势可轻松转移至LPLND。