Klinik III für Innere Medizin, Herzzentrum der Universität zu Köln, Cologne, Germany.
Klinik für Allgemeine und Interventionelle Kardiologie, Herz- und Diabeteszentrum NRW, Bad Oeynhausen, Germany.
ESC Heart Fail. 2024 Jun;11(3):1540-1552. doi: 10.1002/ehf2.14611. Epub 2024 Jan 15.
In pulmonary arterial hypertension (PAH), upfront combination therapy with ERA and PDE5i is associated with a reduction in morbidity and mortality events and improves standard haemodynamics, but data remain limited. Aims of this study were (i) to capture detailed haemodynamic effects of rapid sequential dual combination therapy in patients with newly diagnosed PAH; (ii) to monitor the impact of treatment initiation on clinical variables and patients' risk status, and (iii) to compare the treatment effect in patients with 'classical PAH' and 'PAH with co-morbidities'.
Fifty patients (median age 57 [42-71] years, 66% female) with newly diagnosed PAH (76% idiopathic) were treated with a PD5i/sGC-S or ERA, followed by addition of the respective other drug class within 4 weeks. All patients underwent repeat right heart catheterization (RHC) during early follow-up.
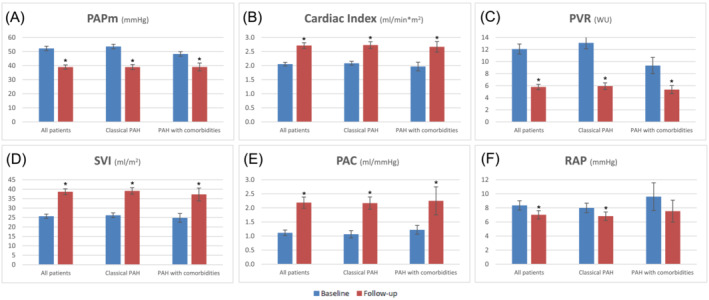
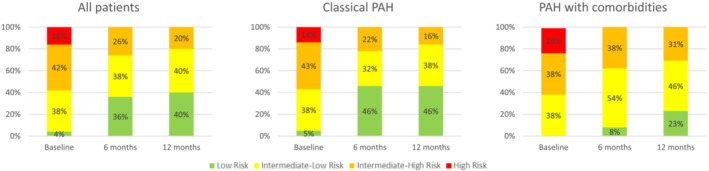
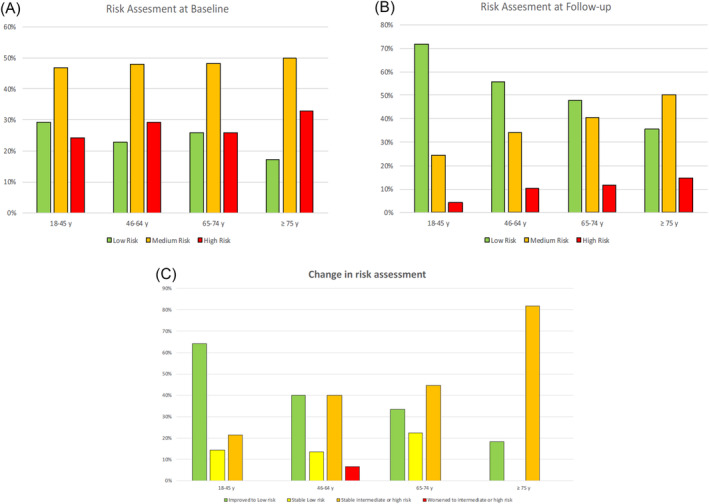
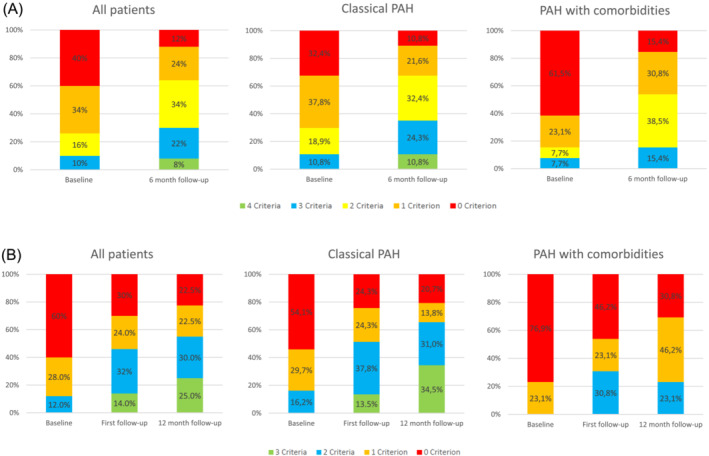
At early repeat RHC (7 ± 2 months), there were substantial reductions in mean pulmonary artery pressure (mPAP: 52.2 ± 13.5 to 39.0 ± 10.6 mmHg; -25.3%), and pulmonary vascular resistance (PVR: 12.1 ± 5.7 to 5.8 ± 3.1 WU; -52.1%), and an increase in cardiac index (2.1 ± 0.4 to 2.7 ± 0.7 mL/min/m; +32.2%) (all P < 0.05). Haemodynamic improvements correlated with improved clinical parameters including 6-min walking distance (336 ± 315 to 389 ± 120 m), NTproBNP levels (1.712 ± 2.024 to 506 ± 550 ng/L, both P < 0.05) and WHO-FC at 12 months, resulting in improved risk status, and were found in patients with few (n = 37) or multiple cardiovascular co-morbidities (BMI > 30 kg/m, hypertension, diabetes, coronary artery disease [≥3]; n = 13), albeit baseline PVR in PAH patients with multiple co-morbidities was lower (9.3 ± 4.4 vs. 13.1 ± 5.9 WU) and PVR reduction less pronounced compared with those with few co-morbidities (-42.7% vs. -54.7%). However, comprehensive haemodynamic assessment considering further variables of prognostic relevance such as stroke volume index and pulmonary artery compliance showed similar improvements among the two groups (SVI: +50.0% vs. +49.2%; PA: 91.7% vs. 100.0%). Finally, the 4-strata risk assessment approach was better able to capture treatment response as compared with other approaches, particularly in patients with co-morbidities.
Rapid sequential combination therapy with PDE5i/sGC-S and ERA substantially ameliorates cardiopulmonary haemodynamics at early follow-up in patients without, and to a lesser extent, with cardiovascular co-morbidities. This occurs in line with improvements of clinical parameters and risk status.
在肺动脉高压(PAH)中,ERA 和 PDE5i 的联合治疗可降低发病率和死亡率事件,并改善标准血液动力学,但数据仍然有限。本研究的目的是:(i)在新诊断的 PAH 患者中,快速序贯双重联合治疗的详细血液动力学效应;(ii)监测治疗启动对临床变量和患者风险状况的影响;(iii)比较“经典 PAH”和“伴有合并症的 PAH”患者的治疗效果。
50 例新诊断的 PAH 患者(中位年龄 57[42-71]岁,66%为女性)接受 PD5i/sGC-S 或 ERA 治疗,随后在 4 周内添加各自的另一种药物类别。所有患者在早期随访期间均接受重复右心导管检查(RHC)。
在早期重复 RHC(7±2 个月)时,平均肺动脉压(mPAP:52.2±13.5 至 39.0±10.6mmHg;-25.3%)和肺血管阻力(PVR:12.1±5.7 至 5.8±3.1WU;-52.1%)显著降低,心指数(2.1±0.4 至 2.7±0.7mL/min/m;+32.2%)增加(均 P<0.05)。血液动力学的改善与临床参数的改善相关,包括 6 分钟步行距离(336±315 至 389±120m)、NTproBNP 水平(1.712±2.024 至 506±550ng/L,均 P<0.05)和 12 个月时的 WHO-FC,导致风险状况改善,并且在有或没有几种心血管合并症(BMI>30kg/m2、高血压、糖尿病、冠状动脉疾病[≥3];n=13)的患者中均可观察到,尽管有多种合并症的 PAH 患者的基线 PVR 较低(9.3±4.4 与 13.1±5.9WU),并且与仅有几种合并症的患者相比,PVR 降低幅度较小(-42.7%与-54.7%)。然而,考虑到与预后相关的其他变量,如每搏量指数和肺动脉顺应性,综合血液动力学评估显示两组之间具有相似的改善(SVI:+50.0%与+49.2%;PA:91.7%与 100.0%)。最后,4 层风险评估方法能够更好地捕捉治疗反应,尤其是在伴有合并症的患者中。
在无心血管合并症和较少心血管合并症的患者中,PDE5i/sGC-S 和 ERA 的快速序贯联合治疗可在早期随访中显著改善心肺血液动力学。这与临床参数和风险状况的改善有关。