Department of Anaesthesia and Intensive Care, Univ. Grenoble Alpes, Centre Hospitalier Universitaire Grenoble, and Inserm, U1216, Grenoble Institut Neurosciences, 38000, Grenoble, France.
Department of Intensive Care, Hôpital Universitaire de Bruxelles (HUB), Université Libre de Bruxelles (ULB), Brussels, Belgium.
Eur J Trauma Emerg Surg. 2024 Aug;50(4):1209-1217. doi: 10.1007/s00068-023-02435-1. Epub 2024 Jan 16.
This pilot study aimed to determine the capacity of automated infrared pupillometry (AIP) alone and in combination with transcranial doppler (TCD) on admission to rule out need for intense neuroAQ2 critical care (INCC) in severe traumatic brain injury (TBI).
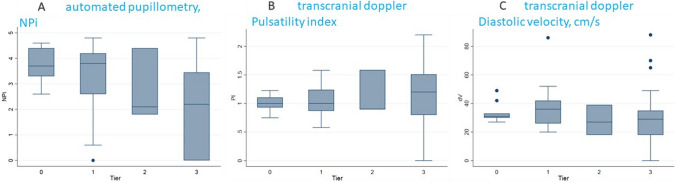
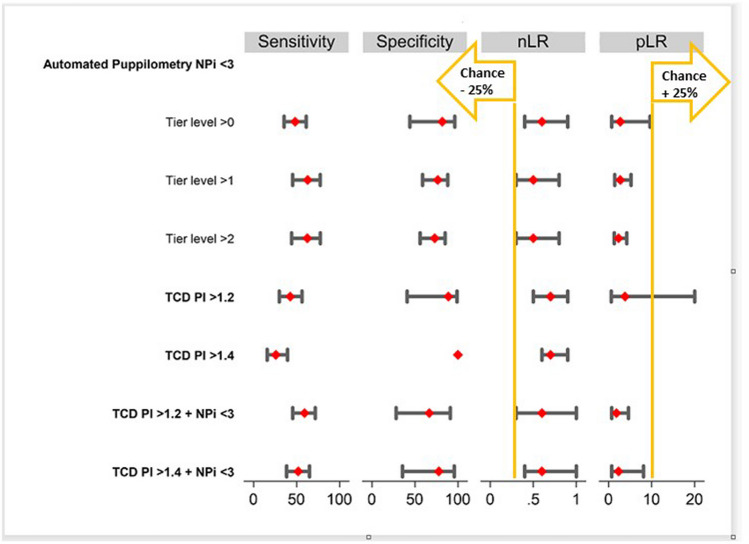
In this observational pilot study clinicians performed AIP and TCD measurements on admission in blunt TBI patients with a Glasgow Coma Score (GCS) < 9 and/or motor score < 6. A Neurological Pupil index (NPi) < 3, Pulsatility Index (PI) > 1,4 or diastolic blood flow velocity (dV) of < 20 cm/s were used to rule out the need for INCC (exceeding the tier 0 Seattle Consensus Conference). The primary outcome was the negative likelihood ratio (nLR) of NPi < 3 alone or in combination with TCD to detect need for INCC.
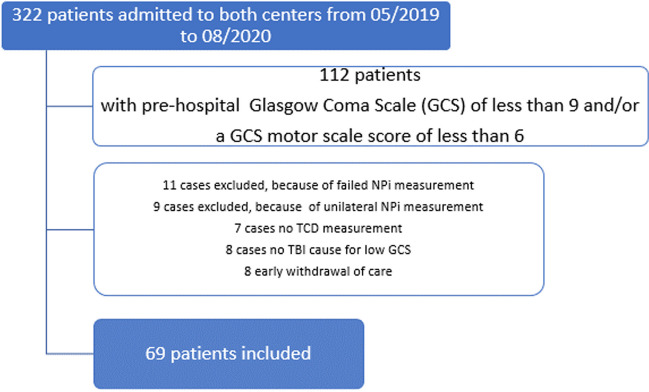
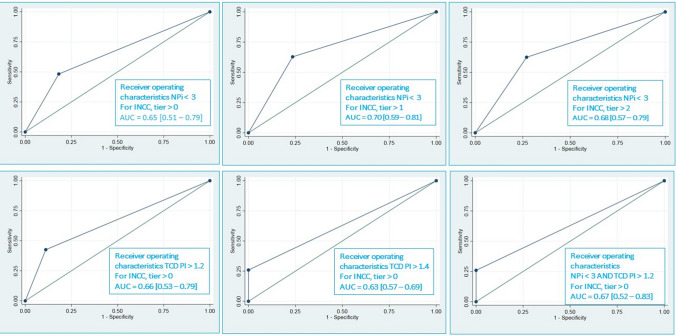
A total of 69 TBI patients were included from May 2019 to September 2020. Of those, 52/69 (75%) median age was 45 [28-67], median prehospital GCS of 7 [5-8], median Injury Severity Scale of 13.0 [6.5-25.5], median Marshall Score of 4 [3-5], the median Glasgow Outcome Scale at discharge was 3 [1-5]. NPi < 3 was an independent predictor of INCC. NPi demonstrated a nLR of 0,6 (95%CI 0.4-0.9; AUROC, 0.65, 95% CI 0.51-0.79), a combination of NPi and TCD showed a nLR of 0.6 (95% CI 0.4-1.0; AUROC 0.67 95% CI 0.52-0.83) to predict INCC.
This pilot study suggests a possible useful contribution of NPi to determine the need for INCC in severe blunt TBI patients on admission.
本研究旨在评估入院时单纯使用自动红外瞳孔测量法(AIP)和结合经颅多普勒超声(TCD)对排除严重创伤性脑损伤(TBI)患者需要接受高强度神经急性质量(INCC)治疗的能力。
本观察性研究中,在格拉斯哥昏迷评分(GCS)<9 和/或运动评分<6 的钝性 TBI 患者入院时,临床医生进行 AIP 和 TCD 测量。使用神经瞳孔指数(NPi)<3、搏动指数(PI)>1.4 或舒张期血流速度(dV)<20cm/s 来排除需要接受 INCC 治疗(超过西雅图共识会议的 0 级)。主要结果是 NPi<3 单独或与 TCD 结合用于检测 INCC 需求的阴性似然比(nLR)。
2019 年 5 月至 2020 年 9 月期间共纳入 69 例 TBI 患者。其中,52/69(75%)中位年龄为 45[28-67]岁,中位院前 GCS 评分为 7[5-8]分,中位损伤严重程度评分 13.0[6.5-25.5]分,中位 Marshall 评分 4[3-5]分,出院时格拉斯哥预后评分中位数为 3[1-5]分。NPi<3 是 INCC 的独立预测因素。NPi 预测 INCC 的 nLR 为 0.6(95%CI 0.4-0.9;AUROC,0.65,95%CI 0.51-0.79),NPi 与 TCD 联合使用预测 INCC 的 nLR 为 0.6(95%CI 0.4-1.0;AUROC 0.67,95%CI 0.52-0.83)。
本研究初步表明,NPi 可能有助于确定严重钝性 TBI 患者入院时是否需要接受 INCC 治疗。