Bhattacharyay Shubhayu, van Leeuwen Florian D, Beqiri Erta, Åkerlund Cecilia A I, Wilson Lindsay, Steyerberg Ewout W, Nelson David W, Maas Andrew I R, Menon David K, Ercole Ari
Division of Anaesthesia, University of Cambridge, Cambridge, UK.
Department of Clinical Neurosciences, University of Cambridge, Cambridge, UK.
Sci Rep. 2025 Jan 2;15(1):95. doi: 10.1038/s41598-024-83862-x.
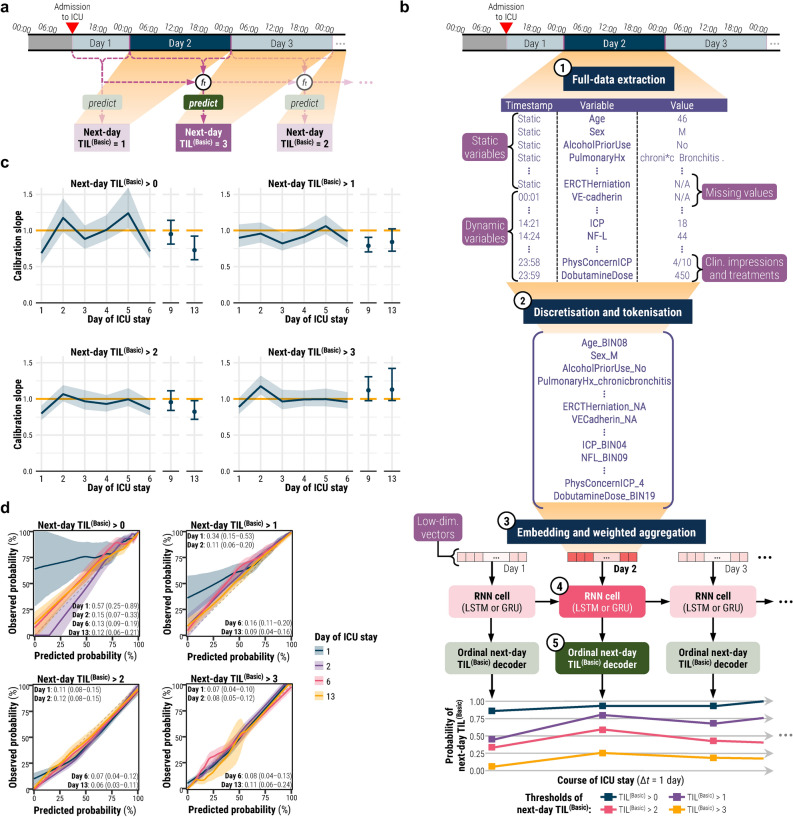
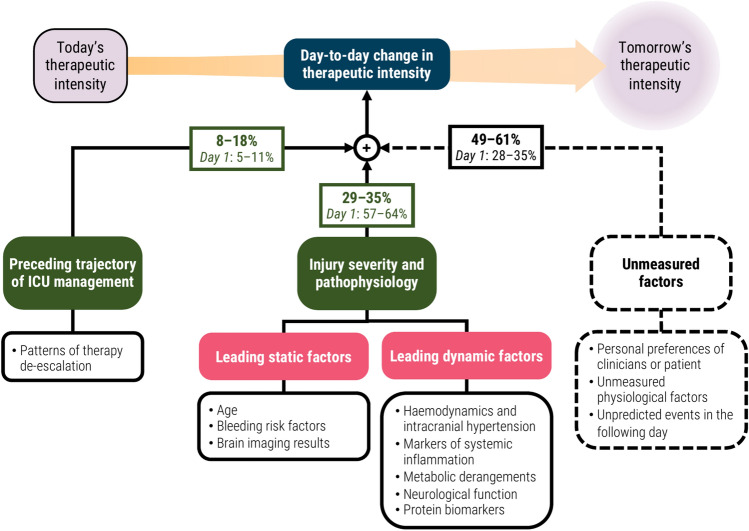
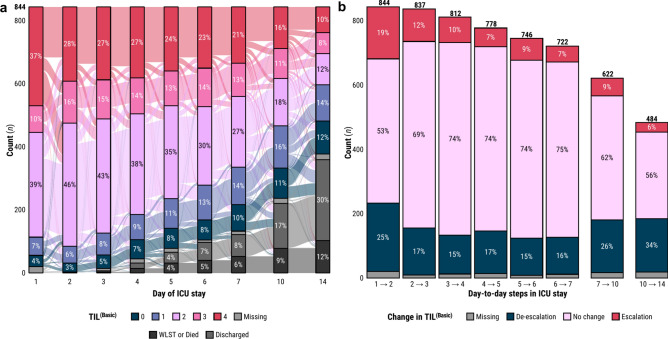
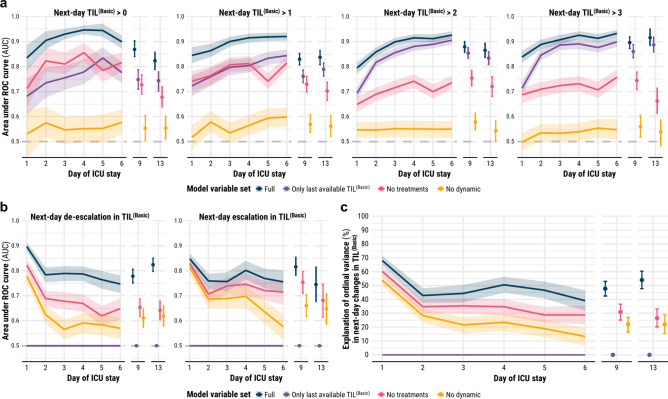
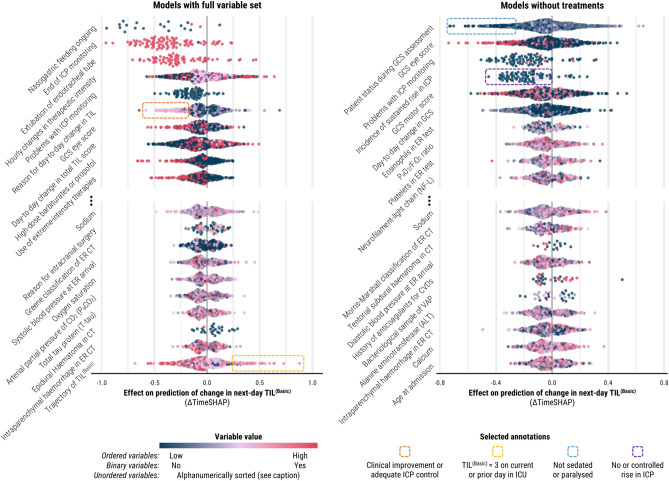
Practices for controlling intracranial pressure (ICP) in traumatic brain injury (TBI) patients admitted to the intensive care unit (ICU) vary considerably between centres. To help understand the rational basis for such variance in care, this study aims to identify the patient-level predictors of changes in ICP management. We extracted all heterogeneous data (2008 pre-ICU and ICU variables) collected from a prospective cohort (n = 844, 51 ICUs) of ICP-monitored TBI patients in the Collaborative European NeuroTrauma Effectiveness Research in TBI study. We developed the TILTomorrow modelling strategy, which leverages recurrent neural networks to map a token-embedded time series representation of all variables (including missing values) to an ordinal, dynamic prediction of the following day's five-category therapy intensity level (TIL) score. With 20 repeats of fivefold cross-validation, we trained TILTomorrow on different variable sets and applied the TimeSHAP (temporal extension of SHapley Additive exPlanations) algorithm to estimate variable contributions towards predictions of next-day changes in TIL. Based on Somers' D, the full range of variables explained 68% (95% CI 65-72%) of the ordinal variation in next-day changes in TIL on day one and up to 51% (95% CI 45-56%) thereafter, when changes in TIL became less frequent. Up to 81% (95% CI 78-85%) of this explanation could be derived from non-treatment variables (i.e., markers of pathophysiology and injury severity), but the prior trajectory of ICU management significantly improved prediction of future de-escalations in ICP-targeted treatment. Whilst there was no significant difference in the predictive discriminability (i.e., area under receiver operating characteristic curve) between next-day escalations (0.80 [95% CI 0.77-0.84]) and de-escalations (0.79 [95% CI 0.76-0.82]) in TIL after day two, we found specific predictor effects to be more robust with de-escalations. The most important predictors of day-to-day changes in ICP management included preceding treatments, age, space-occupying lesions, ICP, metabolic derangements, and neurological function. Serial protein biomarkers were also important and may serve a useful role in the clinical armamentarium for assessing therapeutic needs. Approximately half of the ordinal variation in day-to-day changes in TIL after day two remained unexplained, underscoring the significant contribution of unmeasured factors or clinicians' personal preferences in ICP treatment. At the same time, specific dynamic markers of pathophysiology associated strongly with changes in treatment intensity and, upon mechanistic investigation, may improve the timing and personalised targeting of future care.
重症监护病房(ICU)收治的创伤性脑损伤(TBI)患者的颅内压(ICP)控制方法在不同中心之间差异很大。为了帮助理解这种护理差异的合理依据,本研究旨在确定ICP管理变化的患者层面预测因素。我们从一项前瞻性队列研究(n = 844,51个ICU)中收集的所有异质性数据(2008年ICU前和ICU变量)中提取了ICP监测的TBI患者的数据,该研究是欧洲创伤性脑损伤协作有效性研究。我们开发了TILTomorrow建模策略,该策略利用递归神经网络将所有变量(包括缺失值)的标记嵌入时间序列表示映射到对次日五类治疗强度水平(TIL)评分的有序动态预测。通过20次五折交叉验证,我们在不同的变量集上训练了TILTomorrow,并应用TimeSHAP(Shapley加性解释的时间扩展)算法来估计变量对次日TIL变化预测的贡献。基于Somers' D,全套变量在第一天解释了次日TIL变化中68%(95%CI 65 - 72%)的有序变化,此后随着TIL变化频率降低,解释率高达51%(95%CI 45 - 56%)。高达81%(95%CI 78 - 85%)的这种解释可以从非治疗变量(即病理生理学和损伤严重程度的标志物)中得出,但ICU管理的先前轨迹显著改善了对未来ICP靶向治疗降级的预测。虽然第二天后次日TIL升级(0.80 [95%CI 0.77 - 0.84])和降级(0.79 [95%CI 0.76 - 0.82])之间的预测辨别力(即受试者工作特征曲线下面积)没有显著差异,但我们发现特定的预测因素对降级的影响更稳健。ICP管理每日变化的最重要预测因素包括先前的治疗、年龄、占位性病变、ICP、代谢紊乱和神经功能。系列蛋白质生物标志物也很重要,可能在评估治疗需求的临床手段中发挥有用作用。第二天后TIL每日变化中约一半的有序变化仍无法解释,这突出了未测量因素或临床医生个人偏好在ICP治疗中的重大贡献。同时,与治疗强度变化密切相关的特定病理生理学动态标志物,经机制研究后,可能会改善未来护理的时机和个性化靶向治疗。