IRCCS Humanitas Research Hospital, Via Manzoni 56, 20089, Rozzano, Milan, Italy.
Department of Biomedical Sciences, Humanitas University, via Levi Montalcini 4, Pieve Emanuele, Milan, Italy.
Crit Care. 2024 Jan 16;28(1):23. doi: 10.1186/s13054-023-04785-z.
The use of the passive leg raising (PLR) is limited in acute brain injury (ABI) patients with increased intracranial pressure (ICP) since the postural change of the head may impact on ICP and cerebral autoregulation. However, the PLR use may prevent a positive daily fluid balance, which had been recently associated to worse neurological outcomes. We therefore studied early and delayed effects of PLR on the cerebral autoregulation of patients recovering from ABI.
This is a Prospective, observational, single-center study conducted in critically ill patients admitted with stable ABI and receiving invasive ICP monitoring, multimodal neuromonitoring and continuous hemodynamic monitoring. The fluid challenge consisted of 500 mL of crystalloid over 10 min; fluid responsiveness was defined as cardiac index increase ≥ 10%. Comparisons between different variables at baseline and after PLR were made by paired Wilcoxon signed-rank test. The correlation coefficients between hemodynamic and neuromonitoring variables were assessed using Spearman's rank test.
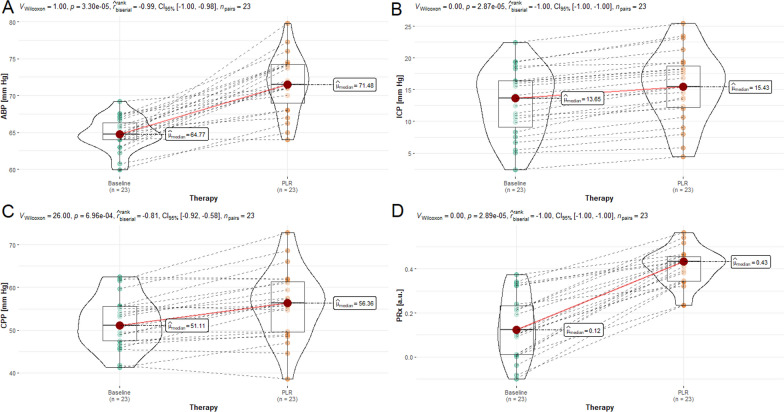
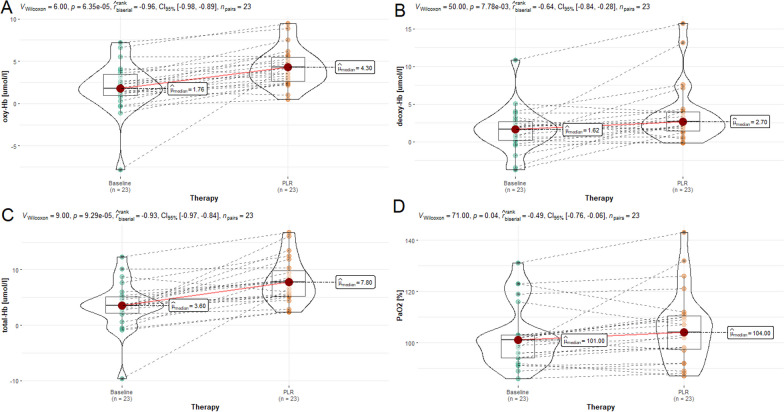
We studied 23 patients [12 patients (52.2%) were fluid responders]. The PLR significantly increased ICP [from 13.7 (8.3-16.4) to 15.4 (12.0-19.2) mmHg; p < 0.001], cerebral perfusion pressure (CPP) [from 51.1 (47.4-55.6) to 56.4 (49.6-61.5) mmHg; p < 0.001] and the pressure reactivity index (PRx) [from 0.12 (0.01-0.24) to 0.43 (0.34-0.46) mmHg; p < 0.001]. Regarding Near Infrared Spectroscopy (NIRS)-derived parameters, PLR significantly increased the arterial component of regional cerebral oxygen saturation (OHbi) [from 1.8 (0.8-3.7) to 4.3 (2.5-5.6) μM cm; p < 0.001], the deoxygenated hemoglobin (HHbi) [from 1.6 (0.2-2.9) to 2.7 (1.4-4.0) μM cm; p = 0.007] and total hemoglobin (cHbi) [from 3.6 (1.9-5.3) to 7.8 (5.2-10.3): p < 0.001]. In all the patients who had altered autoregulation after PLR, these changes persisted ten minutes afterwards. After the PLR, we observed a significant correlation between MAP and CPP and PRx.
In ABI patient with stable ICP, PLR test increased ICP, but mostly within safety values and thresholds. Despite this, cerebral autoregulation was importantly impaired, and this persisted up to 10 min after the end of the maneuvre. Our results discourage the use of PLR test in ABI even when ICP is stable.
由于头部姿势的改变可能会影响颅内压(ICP)和脑自动调节,因此在颅内压升高的急性脑损伤(ABI)患者中,被动抬腿(PLR)的使用受到限制。然而,PLR 的使用可能会防止出现正的每日液体平衡,最近的研究表明这与更差的神经结局相关。因此,我们研究了 PLR 对从 ABI 中恢复的患者脑自动调节的早期和延迟影响。
这是一项前瞻性、观察性、单中心研究,在接受有创 ICP 监测、多模态神经监测和连续血流动力学监测的稳定 ABI 患者中进行。液体挑战由 500 毫升晶体液在 10 分钟内输注完成;血流动力学反应性定义为心指数增加≥10%。使用配对 Wilcoxon 符号秩检验比较基线和 PLR 后的不同变量。使用 Spearman 秩相关检验评估血流动力学和神经监测变量之间的相关系数。
我们研究了 23 名患者[12 名患者(52.2%)为液体反应者]。PLR 显著增加了 ICP[从 13.7(8.3-16.4)mmHg 增加至 15.4(12.0-19.2)mmHg;p<0.001]、脑灌注压(CPP)[从 51.1(47.4-55.6)mmHg 增加至 56.4(49.6-61.5)mmHg;p<0.001]和压力反应性指数(PRx)[从 0.12(0.01-0.24)mmHg 增加至 0.43(0.34-0.46)mmHg;p<0.001]。关于近红外光谱(NIRS)衍生参数,PLR 显著增加了区域脑氧饱和度(OHbi)的动脉成分[从 1.8(0.8-3.7)μM·cm 增加至 4.3(2.5-5.6)μM·cm;p<0.001]、去氧血红蛋白(HHbi)[从 1.6(0.2-2.9)μM·cm 增加至 2.7(1.4-4.0)μM·cm;p=0.007]和总血红蛋白(cHbi)[从 3.6(1.9-5.3)μM·cm 增加至 7.8(5.2-10.3)μM·cm;p<0.001]。在所有 PLR 后自动调节发生改变的患者中,这些变化在 10 分钟后仍然存在。PLR 后,我们观察到 MAP 和 CPP 与 PRx 之间存在显著相关性。
在颅内压稳定的 ABI 患者中,PLR 试验增加了 ICP,但大多仍在安全值和阈值范围内。尽管如此,脑自动调节仍受到严重损害,并且在操作结束后 10 分钟内仍然存在。我们的结果不鼓励在 ICP 稳定时使用 PLR 试验。