Giardina Alberto, Cardim Danilo, Ciliberti Pietro, Battaglini Denise, Ball Lorenzo, Kasprowicz Magdalena, Beqiri Erta, Smielewski Peter, Czosnyka Marek, Frisvold Shirin, Groznik Matjaž, Pelosi Paolo, Robba Chiara
Dipartimento di Scienze Chirurgiche e Diagnostiche, University of Genoa, Genova, Italy.
Department of Neurology, University of Texas Southwestern Medical Center, Dallas, TX, United States.
Front Physiol. 2023 May 2;14:1139658. doi: 10.3389/fphys.2023.1139658. eCollection 2023.
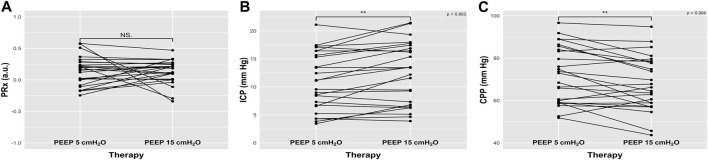
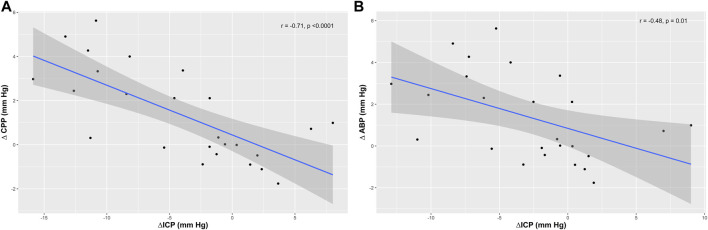
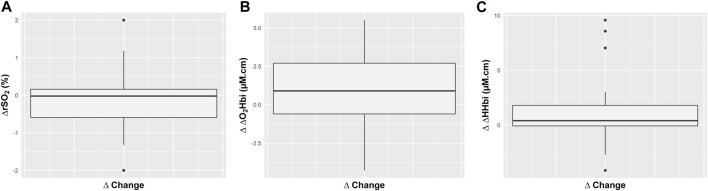
Cerebral autoregulation is the mechanism that allows to maintain the stability of cerebral blood flow despite changes in cerebral perfusion pressure. Maneuvers which increase intrathoracic pressure, such as the application of positive end-expiratory pressure (PEEP), have been always challenged in brain injured patients for the risk of increasing intracranial pressure (ICP) and altering autoregulation. The primary aim of this study is to assess the effect of PEEP increase (from 5 to 15 cmHO) on cerebral autoregulation. Secondary aims include the effect of PEEP increase on ICP and cerebral oxygenation. Prospective, observational study including adult mechanically ventilated patients with acute brain injury requiring invasive ICP monitoring and undergoing multimodal neuromonitoring including ICP, cerebral perfusion pressure (CPP) and cerebral oxygenation parameters obtained with near-infrared spectroscopy (NIRS), and an index which expresses cerebral autoregulation (PRx). Additionally, values of arterial blood gases were analyzed at PEEP of 5 and 15 cmHO. Results are expressed as median (interquartile range). Twenty-five patients were included in this study. The median age was 65 years (46-73). PEEP increase from 5 to 15 cmHO did not lead to worsened autoregulation (PRx, from 0.17 (-0.003-0.28) to 0.18 (0.01-0.24), = 0.83). Although ICP and CPP changed significantly (ICP: 11.11 (6.73-15.63) to 13.43 (6.8-16.87) mm Hg, = 0.003, and CPP: 72.94 (59.19-84) to 66.22 (58.91-78.41) mm Hg, = 0.004), these parameters did not reach clinically relevant levels. No significant changes in relevant cerebral oxygenation parameters were observed. Slow and gradual increases of PEEP did not alter cerebral autoregulation, ICP, CPP and cerebral oxygenation to levels triggering clinical interventions in acute brain injury patients.
脑自动调节是一种机制,它能使脑血流量在脑灌注压发生变化时仍保持稳定。增加胸内压的操作,如应用呼气末正压(PEEP),一直被认为对脑损伤患者存在风险,可能会导致颅内压(ICP)升高并改变自动调节功能。本研究的主要目的是评估PEEP增加(从5cmH₂O增加到15cmH₂O)对脑自动调节的影响。次要目的包括PEEP增加对ICP和脑氧合的影响。这是一项前瞻性观察性研究,纳入了需要有创ICP监测且接受多模态神经监测的成年机械通气急性脑损伤患者,监测内容包括ICP、脑灌注压(CPP)以及通过近红外光谱(NIRS)获得的脑氧合参数,还有一个表示脑自动调节的指标(PRx)。此外,在PEEP为5cmH₂O和15cmH₂O时分析动脉血气值。结果以中位数(四分位间距)表示。本研究共纳入25例患者。中位年龄为65岁(46 - 73岁)。PEEP从5cmH₂O增加到15cmH₂O并未导致自动调节功能恶化(PRx,从0.17(-0.003 - 0.28)变为0.18(0.01 - 0.24),P = 0.83)。尽管ICP和CPP有显著变化(ICP:从11.11(6.73 - 15.63)mmHg变为13.43(从6.8 - 16.87)mmHg,P = 0.003;CPP:从72.94(59.19 - 84)mmHg变为66.22(58.91 - 78.41)mmHg,P = 0.004),但这些参数未达到临床相关水平。未观察到相关脑氧合参数有显著变化。在急性脑损伤患者中,缓慢逐渐增加PEEP不会将脑自动调节、ICP、CPP和脑氧合改变到引发临床干预的水平。