Kotadia Irum D, O'Dowling Robert, Aboagye Akosua, Crawley Richard J, Bodagh Neil, Gharaviri Ali, O'Hare Daniel, Solis-Lemus Jose Alonso, Roney Caroline H, Sim Iain, Ramsey Deborah, Newby David, Chiribiri Amedeo, Plein Sven, Sztriha Laszlo, Scott Paul, Masci Pier-Giorgio, Harrison James, Williams Michelle C, Birns Jonathan, Somerville Peter, Bhalla Ajay, Niederer Steven, O'Neill Mark, Williams Steven E
School of Biomedical Engineering and Imaging Sciences, King's College London London United Kingdom.
Guy's and St Thomas' National Health Service Foundation Trust London United Kingdom.
J Am Heart Assoc. 2024 Feb 6;13(3):e031489. doi: 10.1161/JAHA.123.031489. Epub 2024 Jan 19.
Embolic stroke of unknown source (ESUS) accounts for 1 in 6 ischemic strokes. Current guidelines do not recommend routine cardiac magnetic resonance (CMR) imaging in ESUS, and beyond the identification of cardioembolic sources, there are no data assessing new clinical findings from CMR in ESUS. This study aimed to assess the prevalence of new cardiac and noncardiac findings and to determine their impact on clinical care in patients with ESUS.
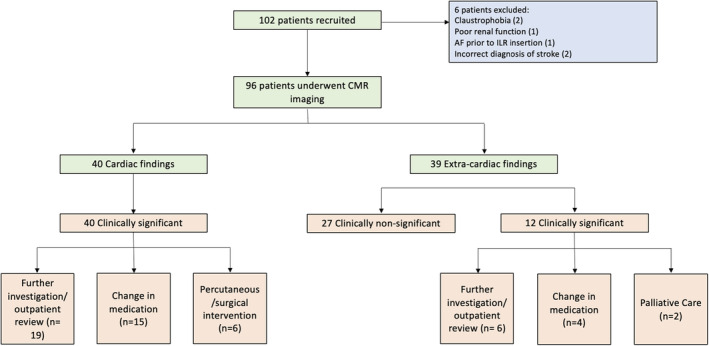
In this prospective, multicenter, observational study, CMR imaging was performed within 3 months of ESUS. All scans were reported according to standard clinical practice. A new clinical finding was defined as one not previously identified through prior clinical evaluation. A clinically significant finding was defined as one resulting in further investigation, follow-up, or treatment. A change in patient care was defined as initiation of medical, interventional, surgical, or palliative care. From 102 patients recruited, 96 underwent CMR imaging. One or more new clinical findings were observed in 59 patients (61%). New findings were clinically significant in 48 (81%) of these patients. Of 40 patients with a new clinically significant cardiac finding, 21 (53%) experienced a change in care (medical therapy, n=15; interventional/surgical procedure, n=6). In 12 patients with a new clinically significant extracardiac finding, 6 (50%) experienced a change in care (medical therapy, n=4; palliative care, n=2).
CMR imaging identifies new clinically significant cardiac and noncardiac findings in half of patients with recent ESUS. Advanced cardiovascular screening should be considered in patients with ESUS.
URL: https://www.clinicaltrials.gov; Unique identifier: NCT04555538.
不明来源栓塞性卒中(ESUS)占缺血性卒中的六分之一。当前指南不建议对ESUS患者进行常规心脏磁共振成像(CMR),除了识别心源性栓塞来源外,尚无数据评估CMR在ESUS中产生的新临床发现。本研究旨在评估新的心脏和非心脏发现的患病率,并确定其对ESUS患者临床治疗的影响。
在这项前瞻性、多中心观察性研究中,于ESUS发生后3个月内进行CMR成像。所有扫描均按照标准临床实践进行报告。新的临床发现定义为先前临床评估未发现的发现。具有临床意义的发现定义为导致进一步检查、随访或治疗的发现。患者治疗的改变定义为开始药物、介入、手术或姑息治疗。从招募的102例患者中,96例接受了CMR成像。59例患者(61%)观察到一个或多个新的临床发现。其中48例(81%)患者的新发现具有临床意义。在40例有新的具有临床意义的心脏发现的患者中,21例(53%)治疗发生改变(药物治疗,n = 15;介入/手术治疗,n = 6)。在12例有新的具有临床意义的心脏外发现的患者中,6例(50%)治疗发生改变(药物治疗,n = 4;姑息治疗,n = 2)。
CMR成像在半数近期ESUS患者中发现了新的具有临床意义的心脏和非心脏发现。对于ESUS患者应考虑进行高级心血管筛查。