Tan Ying, Zhang Ziqi, Zhou Peipei, Zhang Qiling, Li Nan, Yan Qianhua, Huang Liji, Yu Jiangyi
Department of Endocrinology, Jiangsu Province Hospital of Chinese Medicine, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, China.
The First Clinical Medical College, Nanjing University of Chinese Medicine, Nanjing, China.
Front Pharmacol. 2024 Jan 5;14:1288159. doi: 10.3389/fphar.2023.1288159. eCollection 2023.
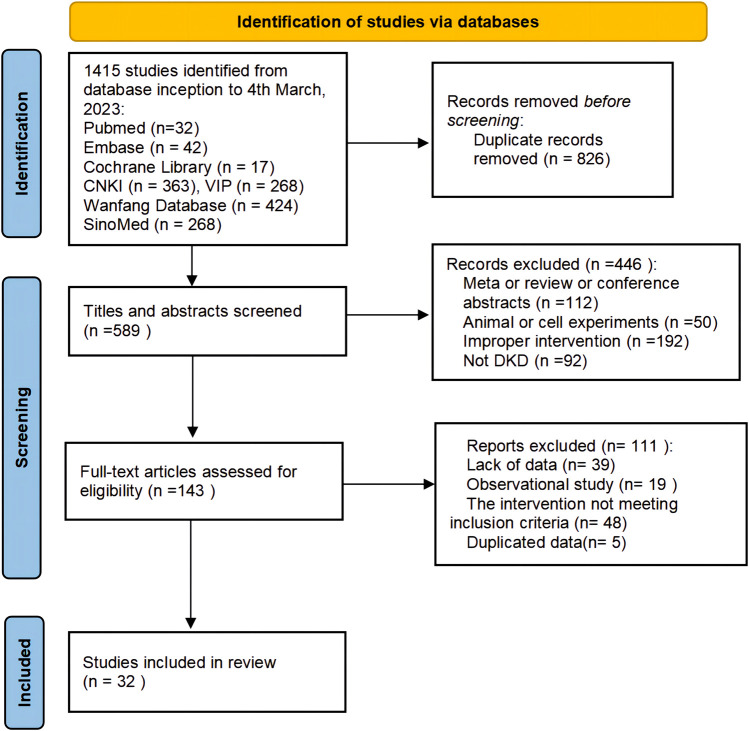
Diabetic kidney disease (DKD) is one of the most serious microvascular complications of diabetes, with the incidence rate increasing yearly, which is the leading cause of chronic kidney disease (CKD) and end-stage kidney disease. Abelmoschus Manihot capsule, as a proprietary Chinese patent medicine, is widely used for treating CKD in China. Currently, the combination of Abelmoschus Manihot (AM) capsule and renin-angiotensin-aldosterone system inhibitor (RASI) has gained popularity as a treatment option for DKD, with more and more randomized control trials (RCTs) in progress. However, the high-quality clinical evidence supporting its application in DKD is still insufficient. To comprehensively and systematically evaluate the efficacy and safety of AM capsule combined with RASI in the treatment of DKD. English and Chinese databases such as Pubmed, Cochrane Library, Embase, CNKI, SinoMed, WF, and VIP were searched to collect the RCTs of AM capsule in treatment of DKD. Then Two investigators independently reviewed and extracted data from the RCTs which met the inclusion criteria. The quality of the data was assessed using the Cochrane risk of bias assessment tool, and meta-analysis was performed using RevMan 5.4 software. 32 RCTs with a total of 2,881 DKD patients (1,442 in the treatment group and 1,439 in the control group) were included. The study results showed that AM capsule combined with RASI could be more effective in decreasing 24h-UTP [MD = -442.05, 95% CI (-609.72, -274.38), < 0.00001], UAER [MD = -30.53, 95% CI (-39.10, -21.96), < 0.00001], UACR [MD = -157.93, 95% CI (-288.60, -27.25), < 0.00001], Scr [MD = -6.80, 95% CI (-9.85, -3.74), < 0.0001], and BUN [MD = -0.59, 95% CI (-1.07, -0.12), = 0.01], compared to using RASI alone. According to the subgroup analyses, the combination of AM and ARB seems to be more effective in reducing UAER than the combination of ACEI, and the addition of AM may achieve a more significant clinical effect on decreasing Scr for DKD patients with 24h-UTP>2 g or Scr>110-133 μmol/L and >133 μmol/L. Furthermore, no additional adverse reactions were observed in the combination group [OR = 1.06; 95%CI: (0.66, 1.69), = 0.82]. Combining AM with RASI may be a superior strategy for DKD treatment compared to RASI monotherapy. However, due to significant heterogeneity, the results should be interpreted with great caution, and more high-quality RCTs with multi-centers, different stages of DKD, large sample sizes, and long follow-up periods are still needed to improve the evidence quality of AM for DKD in the future. https://www.crd.york.ac.uk/PROSPERO/#recordDetails; Identifier CRD42022351422.
糖尿病肾病(DKD)是糖尿病最严重的微血管并发症之一,其发病率逐年上升,是慢性肾脏病(CKD)和终末期肾病的主要原因。秋葵胶囊作为一种中成药,在中国被广泛用于治疗CKD。目前,秋葵(AM)胶囊与肾素-血管紧张素-醛固酮系统抑制剂(RASI)联合使用已成为DKD的一种治疗选择,越来越多的随机对照试验(RCT)正在进行。然而,支持其在DKD中应用的高质量临床证据仍然不足。为了全面、系统地评价AM胶囊联合RASI治疗DKD的疗效和安全性,检索了英文和中文数据库,如Pubmed、Cochrane图书馆、Embase、CNKI、SinoMed、WF和VIP,以收集AM胶囊治疗DKD的RCT。然后,两名研究者独立对符合纳入标准的RCT进行文献回顾和数据提取。采用Cochrane偏倚风险评估工具对数据质量进行评估,并使用RevMan 5.4软件进行荟萃分析。纳入32项RCT,共2881例DKD患者(治疗组1442例,对照组1439例)。研究结果表明,与单独使用RASI相比,AM胶囊联合RASI能更有效地降低24小时尿微量蛋白[MD=-442.05,95%CI(-609.72,-274.38),P<0.00001]、尿白蛋白排泄率(UAER)[MD=-30.53,95%CI(-39.10,-21.96),P<0.00001]、尿白蛋白肌酐比值(UACR)[MD=-157.93,95%CI(-288.60,-27.25),P<0.00001]、血肌酐(Scr)[MD=-6.80,95%CI(-9.85,-3.74),P<0.0001]和尿素氮(BUN)[MD=-0.59,95%CI(-1.07,-0.12),P=0.01]。亚组分析显示,AM与ARB联合使用在降低UAER方面似乎比ACEI联合使用更有效,对于24小时尿微量蛋白>2g或Scr>110-133μmol/L以及>133μmol/L的DKD患者,加用AM在降低Scr方面可能具有更显著的临床效果。此外,联合治疗组未观察到额外的不良反应[OR=1.06;95%CI:(0.66,1.69),P=0.82]。与RASI单药治疗相比,AM与RASI联合使用可能是治疗DKD的更佳策略。然而,由于存在显著异质性,对结果的解释应极为谨慎,未来仍需要更多多中心、不同DKD阶段、大样本量和长期随访的高质量RCT,以提高AM治疗DKD的证据质量。https://www.crd.york.ac.uk/PROSPERO/#recordDetails;标识符CRD42022351422